

Evolving role of bone biomarkers in castration-resistant prostate cancer
- PMID: 20824045
- PMCID: PMC2933689
- DOI: 10.1593/neo.10610
Evolving role of bone biomarkers in castration-resistant prostate cancer
Abstract
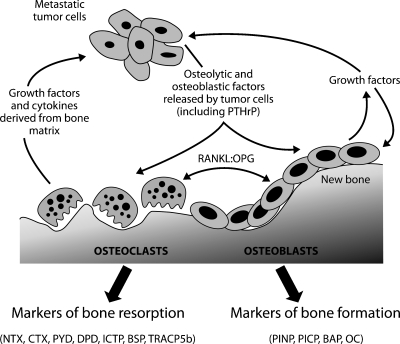
The preferential metastasis of prostate cancer cells to bone disrupts the process of bone remodeling and results in lesions that cause significant pain and patient morbidity. Although prostate-specific antigen (PSA) is an established biomarker in prostate cancer, it provides only limited information relating to bone metastases and the treatment of metastatic bone disease with bisphosphonates or novel noncytotoxic targeted or biological agents that may provide clinical benefits without affecting PSA levels. As bone metastases develop, factors derived from bone metabolism are released into blood and urine, including N- and C-terminal peptide fragments of type 1 collagen and bone-specific alkaline phosphatase, which represent potentially useful biomarkers for monitoring metastatic bone disease. A number of clinical trials have investigated these bone biomarkers with respect to their diagnostic, prognostic, and predictive values. Results suggest that higher levels of bone biomarkers are associated with an increased risk of skeletal-related events and/or death. As a result of these findings, bone biomarkers are now being increasingly used as study end points, particularly in studies investigating novel agents with putative bone effects. Data from prospective clinical trials are needed to validate the use of bone biomarkers and to confirm that marker levels provide additional information beyond traditional methods of response evaluation for patients with metastatic prostate cancer.
Figures
References
-
- Ferlay J, Autier P, Boniol M, Heanue M, Colombet M, Boyle P. Estimates of the cancer incidence and mortality in Europe in 2006. Ann Oncol. 2007;18:581–592. - PubMed
-
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin. 2009;59:225–249. - PubMed
-
- Sternberg CN. Systemic chemotherapy and new experimental approaches in the treatment of metastatic prostate cancer. Ann Oncol. 2008;19:vii91–vii95. - PubMed
-
- Scher HI, Halabi S, Tannock I, Morris M, Sternberg CN, Carducci MA, Eisenberger MA, Higano C, Bubley GJ, Dreicer R, et al. Design and end points of clinical trials for patients with progressive prostate cancer and castrate levels of testosterone: recommendations of the Prostate Cancer Clinical Trials Working Group. J Clin Oncol. 2008;26:1148–1159. - PMC - PubMed
-
- Bubendorf L, Schopfer A, Wagner U, Sauter G, Moch H, Willi N, Gasser TC, Mihatsch MJ. Metastatic patterns of prostate cancer: an autopsy study of 1,589 patients. Hum Pathol. 2000;31:578–583. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous