

Direct costs of care in a randomized controlled trial of endoscopic sclerotherapy versus emergency portacaval shunt for bleeding esophageal varices in cirrhosis--Part 4
- PMID: 20824373
- PMCID: PMC3023018
- DOI: 10.1007/s11605-010-1332-6
Direct costs of care in a randomized controlled trial of endoscopic sclerotherapy versus emergency portacaval shunt for bleeding esophageal varices in cirrhosis--Part 4
Abstract
Background: Emergency treatment of bleeding esophageal varices (BEV) in cirrhotic patients is of prime importance because of the high mortality rate surrounding the episode of acute bleeding. Nevertheless, there is a paucity of randomized controlled trials of emergency surgical therapy and no reports of the costs of any of the widely used forms of emergency treatment. The important issue of direct costs of care was examined in a randomized controlled trial that compared endoscopic sclerotherapy (EST) to emergency portacaval shunt (EPCS).
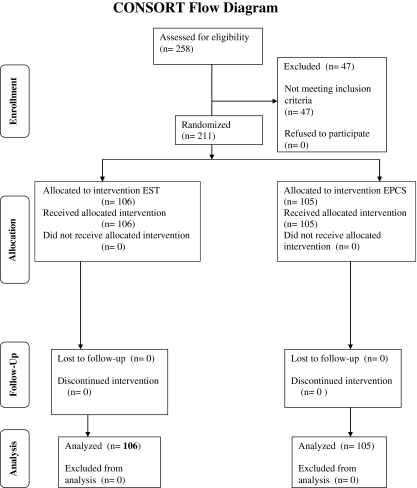
Methods: Two hundred eleven unselected consecutive patients with ultimately biopsy-proven cirrhosis and endoscopically proven acute BEV were randomized to EST (n = 106) or EPCS (n = 105). Diagnostic workup was completed, and EST or EPCS was initiated within 8 h. Criteria for failure of EST or EPCS were clearly defined, and crossover rescue treatment was applied, when primary therapy failed. Ninety-six percent of patients underwent more than 10 years follow-up, or until death. Complete charges for all aspects of care were obtained continuously for more than 10 years.
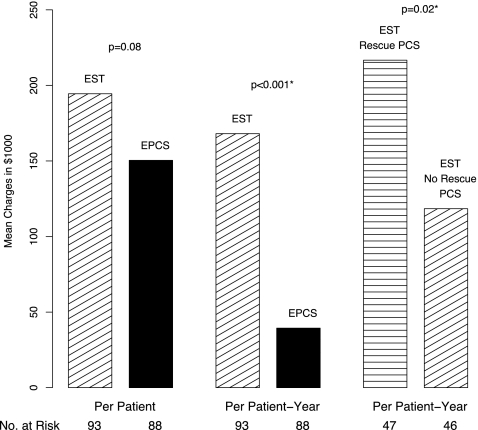
Results: Direct charges for all aspects of care were significantly lower in patients treated by EPCS than in patients treated by emergency EST followed by long-term repetitive sclerotherapy. Charges per patient, per year of treatment, and per year in each child's risk class were significantly lower in patients randomized to EPCS. Charges in patients who failed endoscopic sclerotherapy and underwent a rescue portacaval shunt were significantly higher than the charges in both the unshunted sclerotherapy patients and the patients randomized to EPCS. This result was particularly noteworthy given the widespread practice of using surgical portacaval shunt as rescue treatment only when all other forms of therapy have failed.
Conclusions: In this randomized controlled trial of emergency treatment of acute BEV, EPCS was significantly superior to EST with regard to direct costs of care as reflected in charges for care as well as in survival rate, control of bleeding, and incidence of portal-systemic encephalopathy. These results provide support for the use of EPCS as a first line of emergency treatment of BEV in cirrhosis.
Trial registration: ClinicalTrials.gov NCT00690027.
Figures
References
-
- Orloff MJ. Portal hypertension and portacaval shunt. In: Souba W, Wilmore D, editors. Surgical research. San Diego: Harcourt Brace; 2001. pp. 637–701.
-
- Orloff MJ, Isenberg JI, Wheeler HO, Haynes KS, Jinich-Brook H, Rapier R, Vaida F, Hye RJ. Randomized trial of emergency endoscopic sclerotherapy versus emergency portacaval shunt for acutely bleeding esophageal varices in cirrhosis. J Am Coll Surg. 2009;209:25–45. doi: 10.1016/j.jamcollsurg.2009.02.059. - DOI - PMC - PubMed
-
- Orloff MJ, Isenberg JI, Wheeler HO, Haynes KS, Jinich-Brook H, Rapier R, Vaida F, Hye RJ. Portal-systemic encephalopathy in a randomized controlled trial of endoscopic sclerotherapy versus emergency portacaval shunt treatment of acutely bleeding esophageal varices in cirrhosis. Ann Surg. 2009;250:598–610. - PubMed
-
- Orloff MJ, Isenberg JI, Wheeler HO, Haynes KS, Jinich-Brook H, Rapier R, Vaida F, Hye RJ. Emergency portacaval shunt versus rescue portacaval shunt in a randomized controlled trial of emergency treatment of acutely bleeding esophageal varices in cirrhosis—Part 3. J Gastrointest Surg 2010; in press. - PMC - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
