

HIV-infected patients and treatment outcomes: an equivalence study of community-located, primary care-based HIV treatment vs. hospital-based specialty care in the Bronx, New York
- PMID: 20824549
- PMCID: PMC3005960
- DOI: 10.1080/09540121.2010.484456
HIV-infected patients and treatment outcomes: an equivalence study of community-located, primary care-based HIV treatment vs. hospital-based specialty care in the Bronx, New York
Abstract
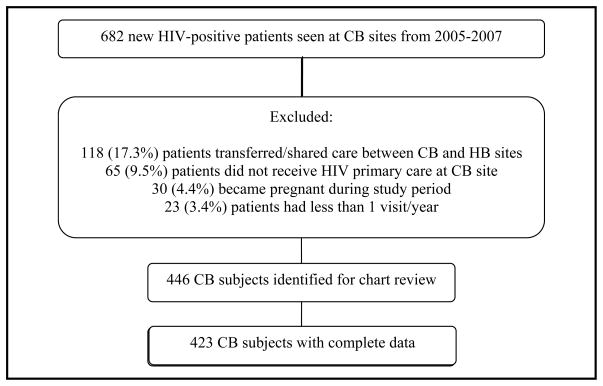
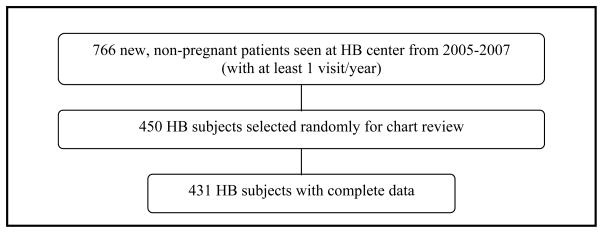
The HIV-infected population in the USA is expanding as patients survive longer and new infections are identified. In many areas, particularly rural/medically underserved regions, there is a growing shortage of providers with sufficient HIV expertise. HIV services incorporated into community-based (CB), primary care settings may therefore improve the distribution and delivery of HIV treatment. Our objective was to describe/compare patients and treatment outcomes in two settings: a community-located, primary care-based HIV program, and a hospital-based (HB) specialty center. CB providers had on-site access to generalist HIV experts. The hospital center was staffed primarily by infectious disease physicians. This was a retrospective cohort study of 854 HIV-positive adults initiating care between 1/2005 and 12/2007 within an academic medical center network in the Bronx, NY. Treatment outcomes were virologic and immunologic response at 16-32 and 48 weeks, respectively, after combination antiretroviral therapy (cART) initiation. We found that HB subjects presented with a higher prevalence of AIDS (59% vs. 46%, p<0.01) and lower initial CD4 (385 vs. 437, p<0.05) than CB subjects. Among 178 community vs. 237 hospital subjects starting cART, 66% vs. 62% achieved virologic suppression (95% confidence interval (CI) difference -0.14-0.06) and 49% vs. 59% achieved immunologic success, defined as a 100 cell/mm³ increase in CD4 (95% CI difference 0.00-0.19). The multivariate-adjusted likelihoods of achieving viral suppression [OR=1.24 (95% CI 0.69-2.33)] and immunologic success [OR=0.76 (95% CI 0.47-1.21)] were not statistically significant for community vs. hospital subjects. Because this was an observational study, propensity scores were used to address potential selection bias when subjects presented to a particular setting. In conclusion, HIV-infected patients initiate care at CB clinics earlier and with less advanced HIV disease. Treatment outcomes are comparable to those at a HB specialty center, suggesting that HIV care can be delivered effectively in community settings.
Figures
References
-
- Blanchard E, Klibanov OM, Axelrod P, Palermo B, Samuel R. Virologic success in an urban HIV clinic: outcome at 12 months in patients who were HAART naïve. HIV Clin Trials. 2008;9:186–191. - PubMed
-
- Branson BM, Handsfield HH, Lampe MA, Janssen RS, Taylor AW, Lyss CB, et al. CDC. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR. 2006;55(RR–14):1–17. - PubMed
-
- Brown TT, Cole SR, Li X, Kingsley LA, Palella FJ, Riddler SA, et al. Antiretroviral therapy and the prevalence and incidence of diabetes mellitus in the multicenter AIDS cohort study. Arch Intern Med. 2005;165:1179–84. - PubMed
-
- Centers for Disease Control and Prevention. HIV Prevalence Estimates—United States, 2006. MMWR. 2008;57:1073–76. - PubMed
-
- Cohn SE, Berk ML, Berry SH, Duan N, Frankel MR, Klein JD, et al. The care of HIV-infected adults in rural areas of the United States. J Acquir Immune Defic Syndr. 2001;28:385–92. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials