

Expression of C4.4A at the invasive front is a novel prognostic marker for disease recurrence of colorectal cancer
- PMID: 20825414
- PMCID: PMC11159794
- DOI: 10.1111/j.1349-7006.2010.01674.x
Expression of C4.4A at the invasive front is a novel prognostic marker for disease recurrence of colorectal cancer
Erratum in
- Cancer Sci. 2010 Nov;101(11):2503
Abstract
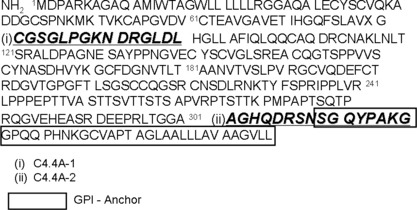
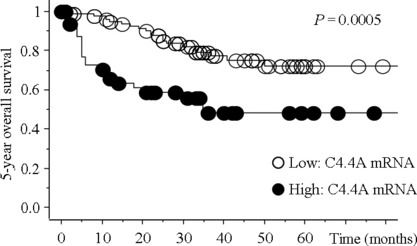
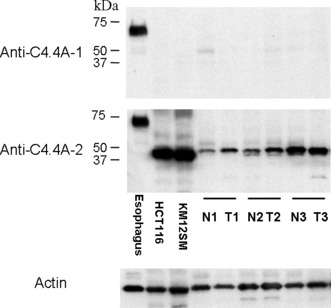
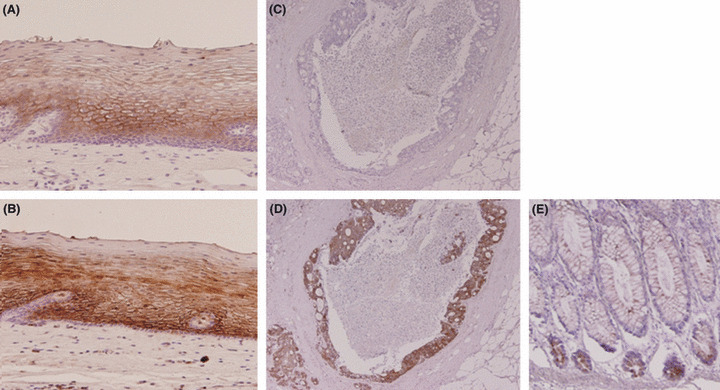
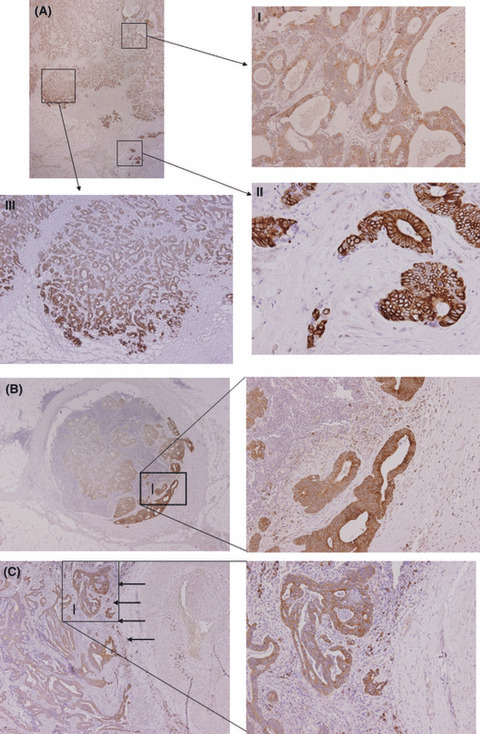
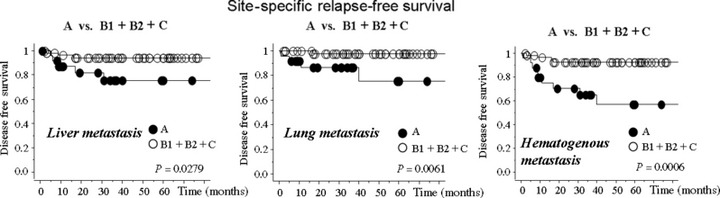
Metastasis-associated gene C4.4A is a glycolipid-anchored membrane protein expressed in several human malignancies. The aim of this study was to explore the expression and clinical relevance of C4.4A in colorectal cancer. By quantitative RT-PCR, 154 colorectal cancer tissues were examined for C4.4A mRNA. We examined 132 colorectal cancer tissues by immunohistochemistry using a new polyclonal antibody that recognizes the C4.4A protein C-terminus containing the glycosylphosphatidyl-inositol anchor signaling sequence. A significant difference in 5-year overall survival was found between samples with high and low expression of C4.4A mRNA (P = 0.0005). Immunohistochemistry showed strong membranous staining of C4.4A at the invasive front of colorectal cancer tumors and at the frontier of metastatic lesions to lymph node and lung. The membranous staining with enhanced intensity at the invasive front of the primary colorectal cancer (Type A: 34/132, 25.6%) was associated with depth of invasion (P = 0.033) and venous invasion (P = 0.003), and was a significant independent prognostic factor (5-year overall survival in the entire series [n = 132; P = 0.004] and disease-free survival in stage II and III colorectal cancers [n = 82; P = 0.003]). Moreover, Type A C4.4A expression was linked to shorter liver metastasis-free survival rate, lung metastasis-free survival rate, or hematogenous metastasis-free survival (P = 0.0279, P = 0.0061, and P = 0.0006, respectively). Our data indicate that expression of the C4.4A protein at the invasive front acts as a novel prognostic marker in colorectal cancer, possibly through invasion-related mechanisms.
© 2010 Japanese Cancer Association.
Figures


References
-
- National Cancer Institute . Colon and rectal cancers. [Cited July 1, 2009.] Available from URL: http://www.cancer.gov/cancertopics/types/colon‐and‐rectal.
-
- Wadhawan A, Stephens R, Adams R. Intermittent therapy in the palliative treatment of metastatic colorectal cancer. Expert Rev Anticancer Ther 2009; 9: 125–34. - PubMed
-
- Hurwitz H, Fehrenbacher L, Novotny W et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med 2004; 350: 2335–42. - PubMed
-
- Van Cutsem E, Köhne CH, Hitre E et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med 2009; 360: 1408–17. - PubMed
-
- Matzku S, Wenzel A, Liu S, Zöller M. Antigenic differences between metastatic and nonmetastatic BSp73 rat tumor variants characterized by monoclonal antibodies. Cancer Res 1989; 49: 1294–9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
