

A severity scoring system for risk assessment of patients with cardiogenic shock: a report from the SHOCK Trial and Registry
- PMID: 20826251
- PMCID: PMC4229030
- DOI: 10.1016/j.ahj.2010.06.024
A severity scoring system for risk assessment of patients with cardiogenic shock: a report from the SHOCK Trial and Registry
Abstract
Background: Early revascularization (ERV) is beneficial in the management of cardiogenic shock (CS) complicating myocardial infarction. The severity of CS varies widely, and identification of independent risk factors for outcome is needed. The effect of ERV on mortality in different risk strata is also unknown. We created a severity scoring system for CS and used it to examine the potential benefit of ERV in different risk strata using data from the SHOCK Trial and Registry.
Methods: Data from 1,217 patients (294 from the randomized trial and 923 from the registry) with CS due to pump failure were included in a Stage 1 severity scoring system using clinical variables. A Stage 2 scoring system was developed using data from 872 patients who had invasive hemodynamic measurements. The outcome was in-hospital mortality at 30 days.
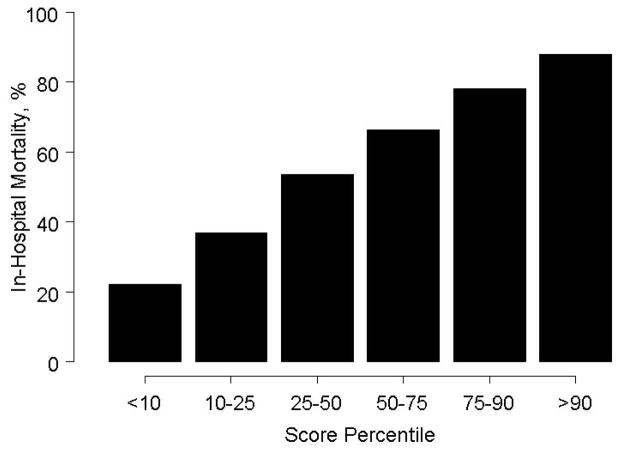
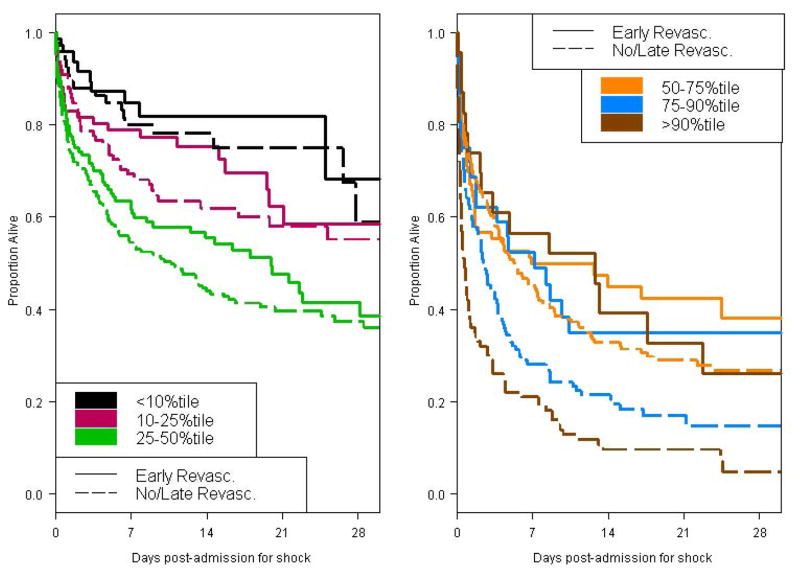
Results: In-hospital mortality at 30 days was 57%. Multivariable modeling identified 8 risk factors (Stage 1): age, shock on admission, clinical evidence of end-organ hypoperfusion, anoxic brain damage, systolic blood pressure, prior coronary artery bypass grafting, noninferior myocardial infarction, and creatinine > or = 1.9 mg/dL (c-statistic = 0.74). Mortality ranged from 22% to 88% by score category. The ERV benefit was greatest in moderate- to high-risk patients (P = .02). The Stage 2 model based on patients with pulmonary artery catheterization included age, end-organ hypoperfusion, anoxic brain damage, stroke work, and left ventricular ejection fraction <28% (c-statistic = 0.76). In this cohort, the effect of ERV did not vary by risk stratum.
Conclusions: Simple clinical predictors provide good discrimination of mortality risk in CS complicating myocardial infarction. Early revascularization is associated with improved survival across a broad range of risk strata.
Trial registration: ClinicalTrials.gov NCT00000552.
2010 Mosby, Inc. All rights reserved.
Figures
Comment in
-
The ancient and often incorrect units for the ventricular stroke work should be replaced by an SI unit.Am Heart J. 2011 Mar;161(3):e9; author reply e11. doi: 10.1016/j.ahj.2010.11.015. Am Heart J. 2011. PMID: 21392594 No abstract available.
References
-
- Berger PB, Holmes DR, Jr, Stebbins AL, et al. Impact of an aggressive invasive catheterization and revascularization strategy on mortality in patients with cardiogenic shock in the Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries (GUSTO-I) trial. An observational study. Circulation. 1997;96(1):122–7. - PubMed
-
- Goldberg RJ, Samad NA, Yarzebski J, et al. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999;340(15):1162–8. - PubMed
-
- Kuhn LA. The treatment of cardiogenic shock. I. The nature of cardiogenic shock. Am Heart J. 1967;74(4):578–81. - PubMed
-
- Lindholm MG, Kober L, Boesgaard S, et al. Cardiogenic shock complicating acute myocardial infarction; prognostic impact of early and late shock development. Eur Heart J. 2003;24(3):258–65. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
