

Prior antiplatelet therapy and outcome following intracerebral hemorrhage: a systematic review
- PMID: 20826714
- PMCID: PMC3013483
- DOI: 10.1212/WNL.0b013e3181f735e5
Prior antiplatelet therapy and outcome following intracerebral hemorrhage: a systematic review
Abstract
Objectives: Antiplatelet therapy (APT) promotes bleeding; therefore, APT might worsen outcome in patients with intracerebral hemorrhage (ICH). We performed a systematic review and meta-analysis to address the hypothesis that pre-ICH APT use is associated with mortality and poor functional outcome following ICH.
Methods: The Medline and Embase databases were searched in February 2008 using relevant key words, limited to human studies in the English language. Cohort studies of consecutive patients with ICH reporting mortality or functional outcome according to pre-ICH APT use were identified. Of 2,873 studies screened, 10 were judged to meet inclusion criteria by consensus of 2 authors. Additionally, we solicited unpublished data from all authors of cohort studies with >100 patients published within the last 10 years, and received data from 15 more studies. Univariate and multivariable-adjusted odds ratios (ORs) for mortality and poor functional outcome were abstracted as available and pooled using a random effects model.
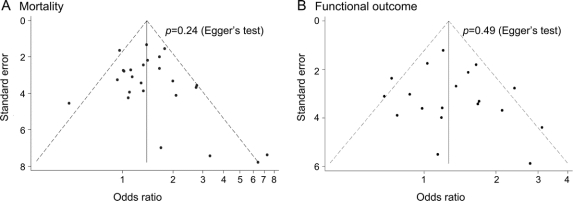
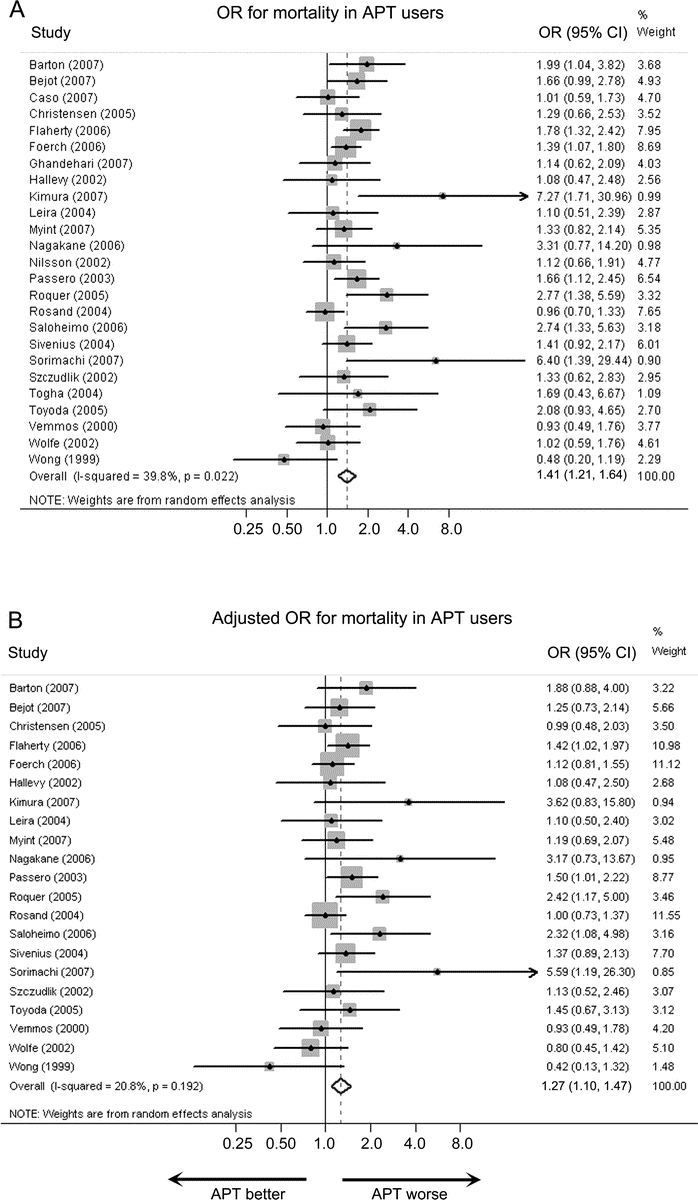
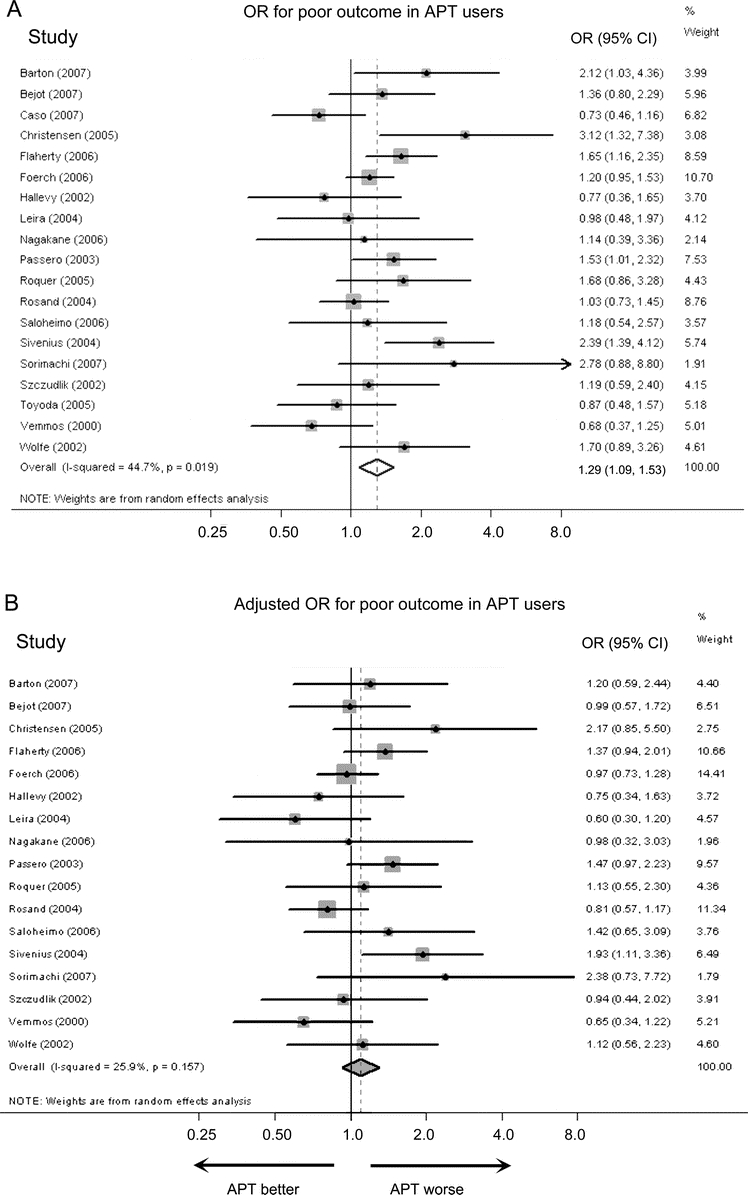
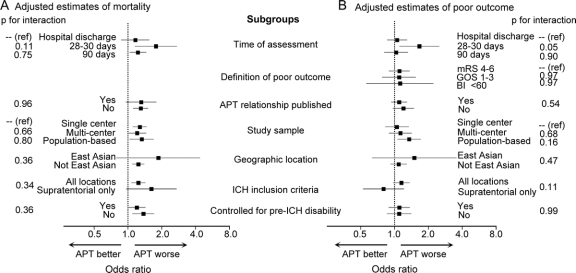
Results: We obtained mortality data from 25 cohorts (15 unpublished) and functional outcome data from 21 cohorts (14 unpublished). Pre-ICH APT users had increased mortality in both univariate (OR 1.41, 95% confidence interval [CI] 1.21 to 1.64) and multivariable-adjusted (OR 1.27, 95% CI 1.10 to 1.47) pooled analyses. By contrast, the pooled OR for poor functional outcome was no longer significant when using multivariable-adjusted estimates (univariate OR 1.29, 95% CI 1.09 to 1.53; multivariable-adjusted OR 1.10, 95% CI 0.93 to 1.29).
Conclusions: In cohort studies, APT use at the time of ICH compared to no APT use was independently associated with increased mortality but not with poor functional outcome.
Figures

Comment in
-
Does antiplatelet therapy at the time of intracerebral hemorrhage bode poor outcome?Neurology. 2010 Oct 12;75(15):1314-5. doi: 10.1212/WNL.0b013e3181f73707. Epub 2010 Sep 15. Neurology. 2010. PMID: 20844242 No abstract available.
-
Prior antiplatelet therapy and outcome following intracerebral hemorrhage: a systematic review.Neurology. 2011 May 3;76(18):1607. doi: 10.1212/WNL.0b013e318219dc1b. Neurology. 2011. PMID: 21536645 No abstract available.
References
-
- Toyoda K, Okada Y, Minematsu K, et al. Antiplatelet therapy contributes to acute deterioration of intracerebral hemorrhage. Neurology 2005;65:1000–1004. - PubMed
-
- Roquer J, Rodriguez Campello A, Gomis M, Ois A, Puente V, Munteis E. Previous antiplatelet therapy is an independent predictor of 30-day mortality after spontaneous supratentorial intracerebral hemorrhage. J Neurol 2005;252:412–416. - PubMed
-
- Saloheimo P, Ahonen M, Juvela S, Pyhtinen J, Savolainen ER, Hillbom M. Regular aspirin-use preceding the onset of primary intracerebral hemorrhage is an independent predictor for death. Stroke 2006;37:129–133. - PubMed
-
- Foerch C, Sitzer M, Steinmetz H, Neumann-Haefelin T. Pretreatment with antiplatelet agents is not independently associated with unfavorable outcome in intracerebral hemorrhage. Stroke 2006;37:2165–2167. - PubMed
-
- Caso V, Paciaroni M, Venti M, et al. Effect of on-admission antiplatelet treatment on patients with cerebral hemorrhage. Cerebrovasc Dis 2007;24:215–218. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical