

Treatment interruption in a primary care antiretroviral therapy program in South Africa: cohort analysis of trends and risk factors
- PMID: 20827216
- PMCID: PMC3024539
- DOI: 10.1097/QAI.0b013e3181f275fd
Treatment interruption in a primary care antiretroviral therapy program in South Africa: cohort analysis of trends and risk factors
Abstract
Objective: To investigate antiretroviral treatment (ART) interruption in a long-term treatment cohort in South Africa.
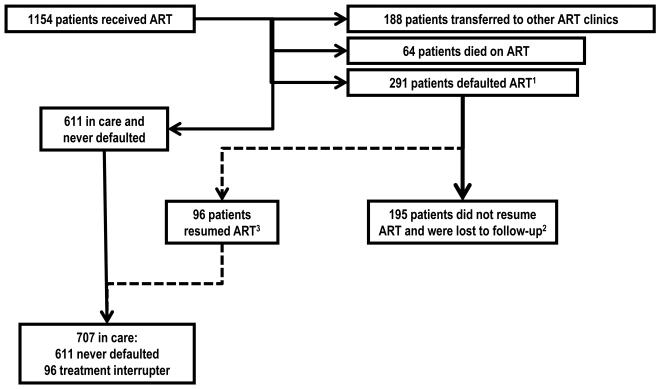
Methods: All adults accessing ART between 2004 and 2009 were included in this analysis. Defaulting was defined as having stopped all ART drugs for more than 30 days. Treatment interrupters were patients who defaulted and returned to care during the study, whereas loss to follow-up was defined as defaulting and not returning to care. Kaplan-Meier estimates and Poisson regression models were used to analyze rates and determinants of defaulting therapy and of treatment resumption.
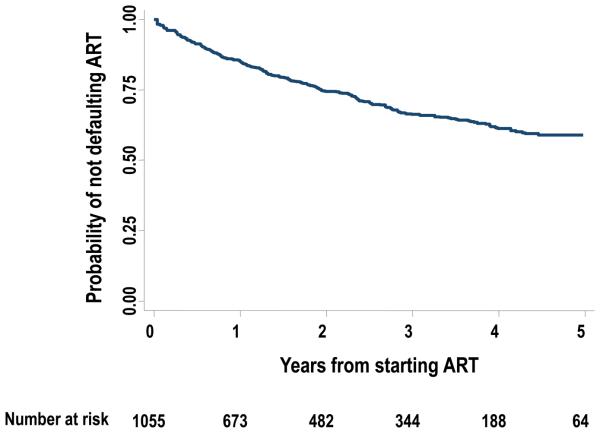
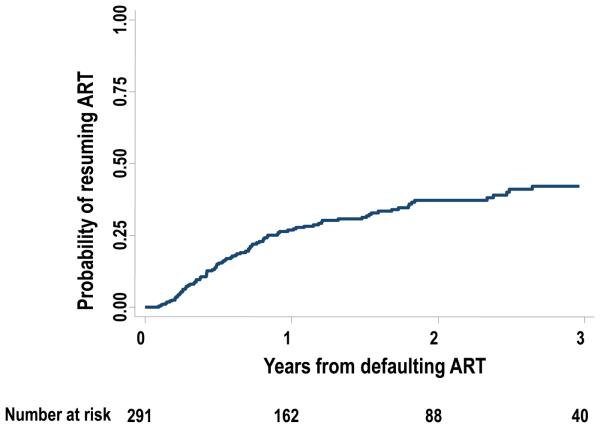
Results: Overall rate of defaulting treatment was 12.8 per 100 person-years (95% confidence interval: 11.4 to 14.4). Risk factors for defaulting were male gender, high baseline CD4 count, recency of ART initiation, and time on ART. The probability of resuming therapy within 3 years of defaulting therapy was 42% (event rate = 21.4 per 100 person-years). Factors associated with restarting treatment were female gender, older age, and time since defaulting.
Conclusions: Defaulting treatment need not be an irreversible event. Interventions to increase retention in care should target men, less immunocompromised patients, and patients during the first 6 months of treatment. Resumption of treatment is most likely within the first year of interrupting therapy.
Figures
References
-
- Towards universal access: scaling up priority HIV/AIDS interventions in the health sector : progress report 2009. World Health Organization; Geneva, Switzerland: 2009. Available from: http://www.who.int/hiv/pub/tuapr_2009_en.pdf last accessed 16/04/2010.
-
- Nachega JB, Mills EJ, Schechter M. Antiretroviral therapy adherence and retention in care in middle-income and low-income countries: current status of knowledge and research priorities. Curr Opin HIV AIDS. Jan;5(1):70–77. - PubMed
-
- Karcher H, Omondi A, Odera J, Kunz A, Harms G. Risk factors for treatment denial and loss to follow-up in an antiretroviral treatment cohort in Kenya. Trop Med Int Health. 2007 May;12(5):687–694. - PubMed
-
- Orrell C, Bangsberg DR, Badri M, Wood R. Adherence is not a barrier to successful antiretroviral therapy in South Africa. Aids. 2003 Jun 13;17(9):1369–1375. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
