

Autoimmune hepatitis: new paradigms in the pathogenesis, diagnosis, and management
- PMID: 20827405
- PMCID: PMC2900560
- DOI: 10.1007/s12072-010-9183-5
Autoimmune hepatitis: new paradigms in the pathogenesis, diagnosis, and management
Abstract
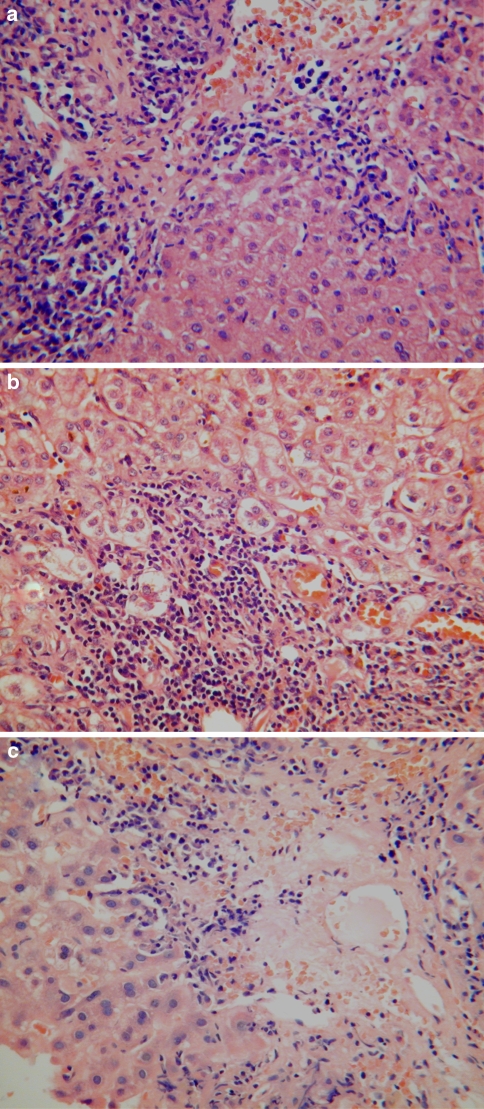
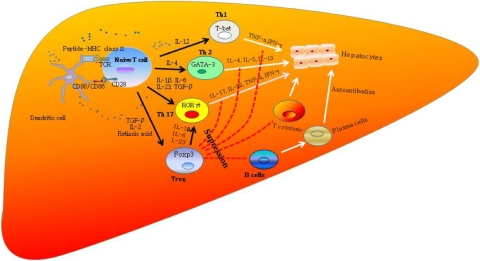
Autoimmune hepatitis (AIH), primary biliary cirrhosis, and primary sclerosing cholangitis are the three major autoimmune diseases affecting the liver, and of these three, AIH is the most typical autoimmune disease being characterized by a T-cell-rich infiltrate, raised circulating γ-globulins, autoantibodies, HLA associations, and links with other autoimmune diseases. It is the only one, of the three diseases, that responds well to immunosuppressive therapy. AIH is caused by dysregulation of immunoregulatory networks and the consequent emergence of autoreactive T cells that orchestrate a progressive destruction of hepatocytes leading untreated to liver failure. T cells play a major role in the immunopathogenesis, and both CD4(+) and CD8(+) T cells are involved together with effector responses mediated by NK cells, γδ T cells, and macrophages. A number of triggering factors have been proposed including viruses, xenobiotics, and drugs, but none have been conclusively shown to be involved in pathogenesis.
Keywords: Autoimmune liver disease; Lymphocytes; Mycophenolate mofetil; Recruitment; Regulatory T cell; Th17.
Figures
Similar articles
-
Autoimmune diseases of the liver and biliary tract and overlap syndromes in childhood.Minerva Gastroenterol Dietol. 2009 Mar;55(1):53-70. Minerva Gastroenterol Dietol. 2009. PMID: 19212308 Review.
-
[Autoimmune liver diseases and their overlap syndromes].Praxis (Bern 1994). 2006 Sep 6;95(36):1363-81. doi: 10.1024/1661-8157.95.36.1363. Praxis (Bern 1994). 2006. PMID: 16989180 Review. German.
-
Paediatric Autoimmune Liver Disease.Dig Dis. 2015;33 Suppl 2:36-46. doi: 10.1159/000440708. Epub 2015 Dec 7. Dig Dis. 2015. PMID: 26641670
-
Aetiopathogenesis of autoimmune hepatitis.World J Gastroenterol. 2008 Jun 7;14(21):3306-12. doi: 10.3748/wjg.14.3306. World J Gastroenterol. 2008. PMID: 18528928 Free PMC article. Review.
-
Autoimmune hepatitis: a comprehensive review.J Autoimmun. 2013 Mar;41:126-39. doi: 10.1016/j.jaut.2012.11.002. Epub 2012 Dec 4. J Autoimmun. 2013. PMID: 23218932 Review.
Cited by
-
CD4+ROR γ t++ and Tregs in a Mouse Model of Diet-Induced Nonalcoholic Steatohepatitis.Mediators Inflamm. 2015;2015:239623. doi: 10.1155/2015/239623. Epub 2015 Jul 1. Mediators Inflamm. 2015. PMID: 26229237 Free PMC article.
-
The Aryl Hydrocarbon Receptor: A Key Bridging Molecule of External and Internal Chemical Signals.Environ Sci Technol. 2015 Aug 18;49(16):9518-31. doi: 10.1021/acs.est.5b00385. Epub 2015 Aug 10. Environ Sci Technol. 2015. PMID: 26079192 Free PMC article. Review.
-
Management of patients with difficult autoimmune hepatitis.Therap Adv Gastroenterol. 2012 Nov;5(6):421-37. doi: 10.1177/1756283X12450251. Therap Adv Gastroenterol. 2012. PMID: 23152735 Free PMC article.
-
Liver homing of clinical grade Tregs after therapeutic infusion in patients with autoimmune hepatitis.JHEP Rep. 2019 Aug 21;1(4):286-296. doi: 10.1016/j.jhepr.2019.08.001. eCollection 2019 Oct. JHEP Rep. 2019. PMID: 32039380 Free PMC article.
-
Evaluation of the effectiveness of treatment with prednisone and azathioprine of autoimmune hepatitis in children.Prz Gastroenterol. 2016;11(1):18-23. doi: 10.5114/pg.2015.52566. Epub 2015 Jun 29. Prz Gastroenterol. 2016. PMID: 27110306 Free PMC article.
References
-
- Czaja AJ, Carpenter HA. Distinctive clinical phenotype and treatment outcome of type 1 autoimmune hepatitis in the elderly. Hepatology. 2006;43(3):532–538. - PubMed
-
- Miyake Y, Iwasaki Y, Sakaguchi K, Shiratori Y. Clinical features of Japanese male patients with type 1 autoimmune hepatitis. Aliment Pharmacol Ther. 2006;24(3):519–523. - PubMed
-
- Al Chalabi T, Boccato S, Portmann BC, Mcfarlane IG, Heneghan MA. Autoimmune hepatitis (AIH) in the elderly: a systematic retrospective analysis of a large group of consecutive patients with definite AIH followed at a tertiary referral centre. J Hepatol. 2006;45(4):575–583. - PubMed
-
- Miyake Y, Iwasaki Y, Terada R, Onishi T, Okamoto R, Sakai N, et al. Clinical characteristics of fulminant-type autoimmune hepatitis: an analysis of eleven cases. Aliment Pharmacol Ther. 2006;23(9):1347–1353. - PubMed
-
- Nikias GA, Batts KP, Czaja AJ. The nature and prognostic implications of autoimmune hepatitis with an acute presentation. J Hepatol. 1994;21(5):866–871. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
