

Objectively measured physical capability levels and mortality: systematic review and meta-analysis
- PMID: 20829298
- PMCID: PMC2938886
- DOI: 10.1136/bmj.c4467
Objectively measured physical capability levels and mortality: systematic review and meta-analysis
Abstract
Objective: To do a quantitative systematic review, including published and unpublished data, examining the associations between individual objective measures of physical capability (grip strength, walking speed, chair rising, and standing balance times) and mortality in community dwelling populations.
Design: Systematic review and meta-analysis.
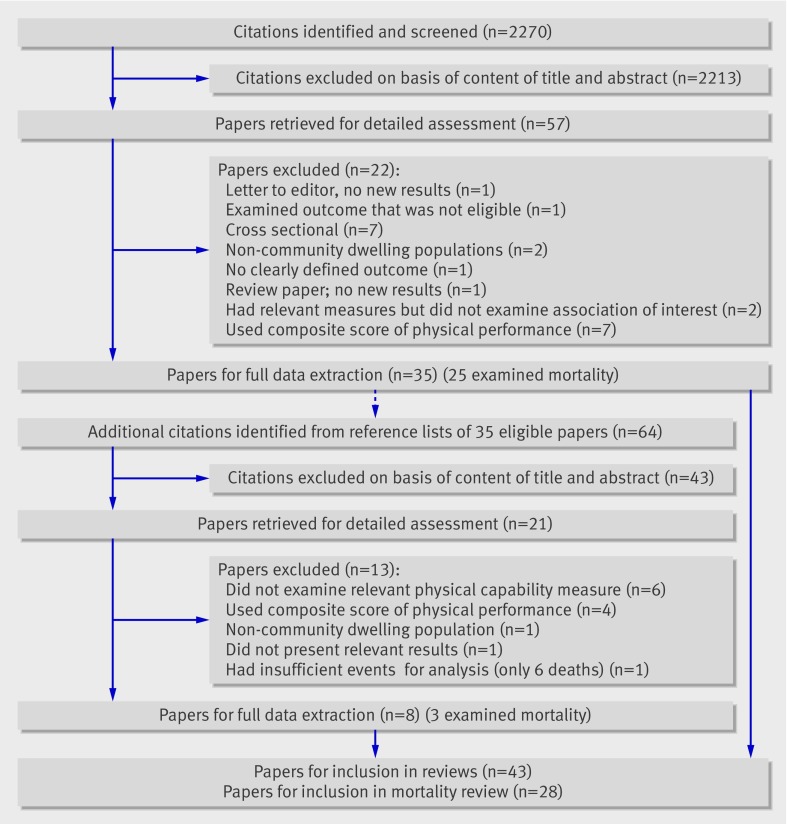
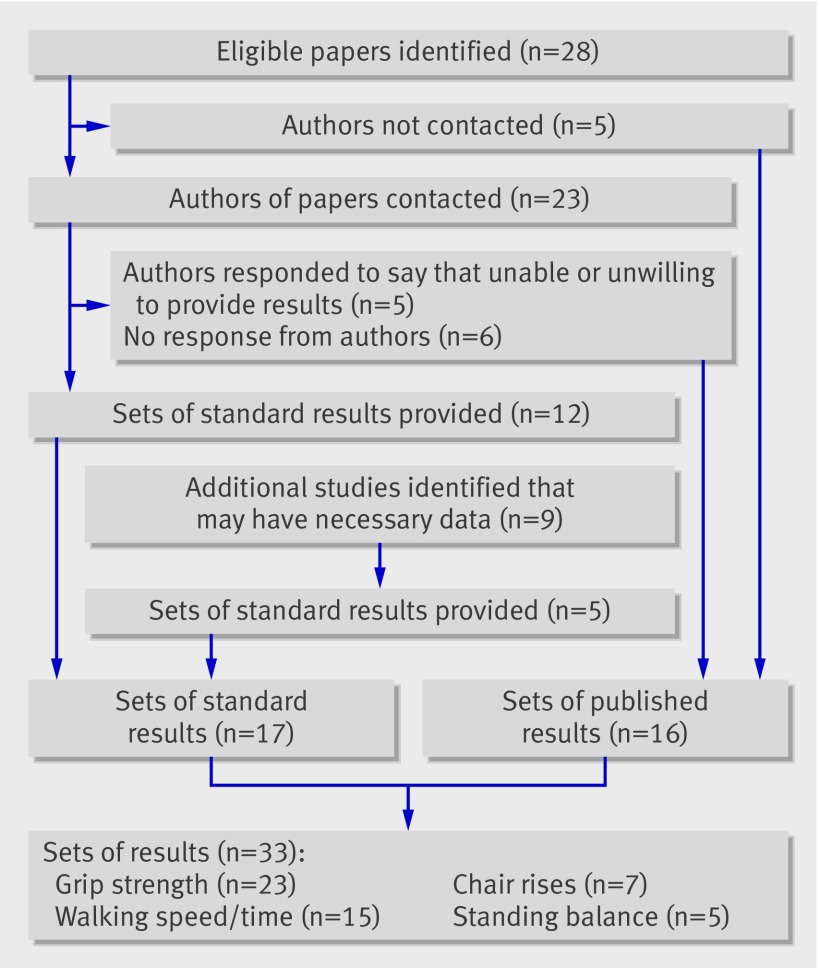
Data sources: Relevant studies published by May 2009 identified through literature searches using Embase (from 1980) and Medline (from 1950) and manual searching of reference lists; unpublished results were obtained from study investigators.
Study selection: Eligible observational studies were those done in community dwelling people of any age that examined the association of at least one of the specified measures of physical capability (grip strength, walking speed, chair rises, or standing balance) with mortality.
Data synthesis: Effect estimates obtained were pooled by using random effects meta-analysis models with heterogeneity between studies investigated.
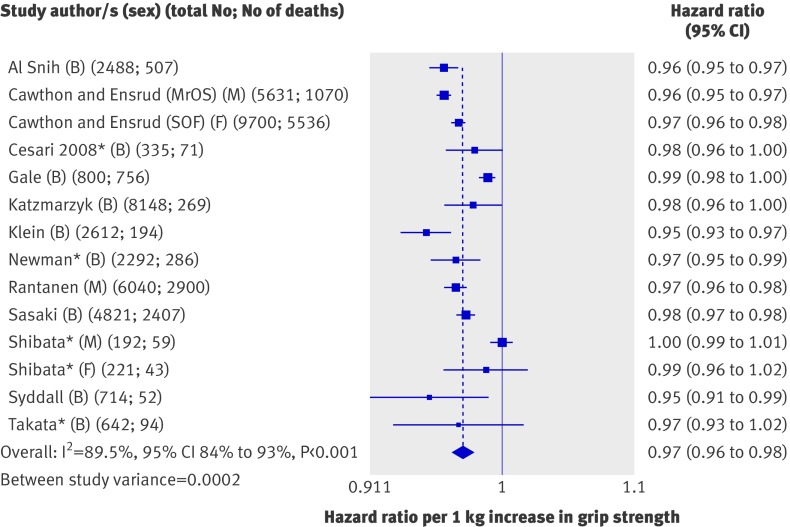
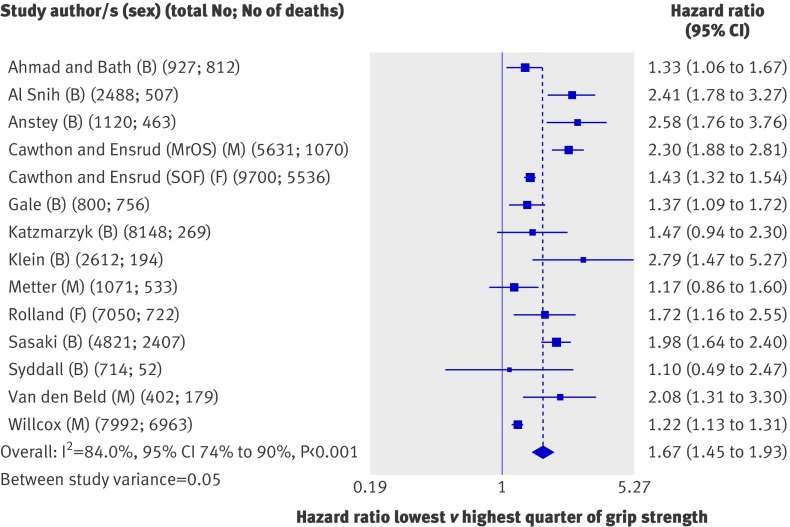
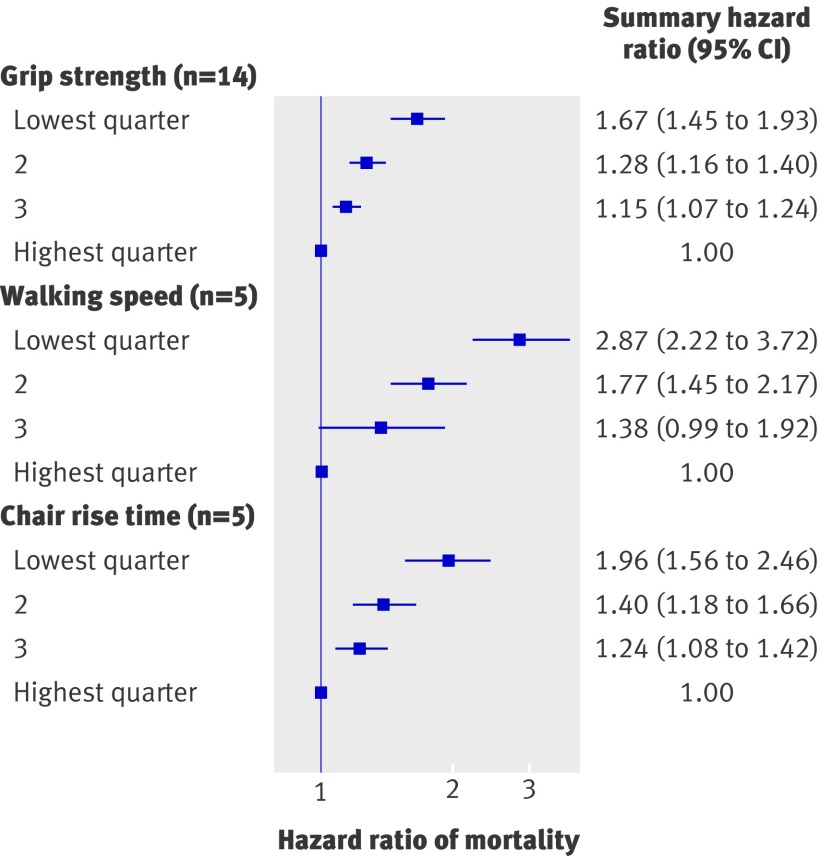
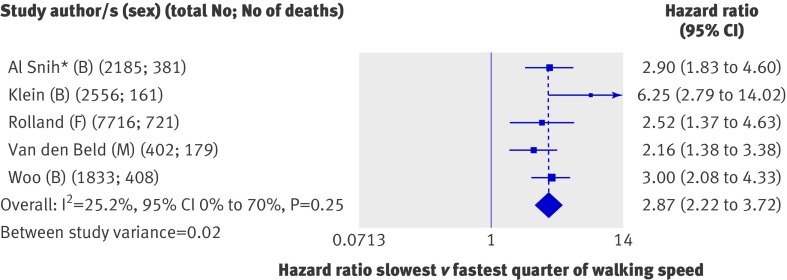
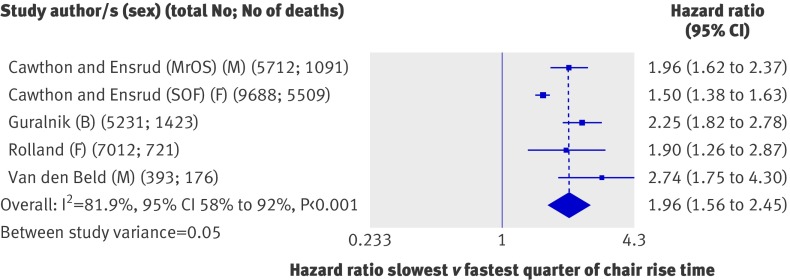
Results: Although heterogeneity was detected, consistent evidence was found of associations between all four measures of physical capability and mortality; those people who performed less well in these tests were found to be at higher risk of all cause mortality. For example, the summary hazard ratio for mortality comparing the weakest with the strongest quarter of grip strength (14 studies, 53 476 participants) was 1.67 (95% confidence interval 1.45 to 1.93) after adjustment for age, sex, and body size (I(2)=84.0%, 95% confidence interval 74% to 90%; P from Q statistic <0.001). The summary hazard ratio for mortality comparing the slowest with the fastest quarter of walking speed (five studies, 14 692 participants) was 2.87 (2.22 to 3.72) (I(2)=25.2%, 0% to 70%; P=0.25) after similar adjustments. Whereas studies of the associations of walking speed, chair rising, and standing balance with mortality have only been done in older populations (average age over 70 years), the association of grip strength with mortality was also found in younger populations (five studies had an average age under 60 years).
Conclusions: Objective measures of physical capability are predictors of all cause mortality in older community dwelling populations. Such measures may therefore provide useful tools for identifying older people at higher risk of death.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Kuh D, New Dynamics of Ageing Preparatory Network. A life course approach to healthy aging, frailty, and capability. J Gerontol A Biol Sci Med Sci 2007;62:717-21. - PubMed
-
- Harwood RH, Conroy SP. Slow walking speed in elderly people. BMJ 2009;339:b4236. - PubMed
-
- Rantanen T. Muscle strength, disability and mortality. Scand J Med Sci Sports 2003;13:3-8. - PubMed
-
- Bohannon RW. Hand-grip dynamometry predicts future outcomes in aging adults. J Geriatr Phys Ther 2008;31:3-10. - PubMed
Publication types
MeSH terms
Grants and funding
- MC_UP_A620_1015/MRC_/Medical Research Council/United Kingdom
- G0600705/MRC_/Medical Research Council/United Kingdom
- MC_U123092721/MRC_/Medical Research Council/United Kingdom
- U01 AR45614/AR/NIAMS NIH HHS/United States
- U01 AR45654/AR/NIAMS NIH HHS/United States
- 2 R01 AG027574-22A1/AG/NIA NIH HHS/United States
- U01-AG027810/AG/NIA NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- EY03083/EY/NEI NIH HHS/United States
- U01 AR45583/AR/NIAMS NIH HHS/United States
- AR35584/AR/NIAMS NIH HHS/United States
- U01 AG18197/AG/NIA NIH HHS/United States
- U01 AR45632/AR/NIAMS NIH HHS/United States
- EY016379/EY/NEI NIH HHS/United States
- 2 R01 AG005394-22A1/AG/NIA NIH HHS/United States
- AG05407/AG/NIA NIH HHS/United States
- AR35582/AR/NIAMS NIH HHS/United States
- UL1 RR024140/RR/NCRR NIH HHS/United States
- U01 AR45647/AR/NIAMS NIH HHS/United States
- AG05394/AG/NIA NIH HHS/United States
- R01 AG027576-22/AG/NIA NIH HHS/United States
- MC_U123092724/MRC_/Medical Research Council/United Kingdom
- AR35583/AR/NIAMS NIH HHS/United States
- R01 AG005407/AG/NIA NIH HHS/United States
- U01 AR45580/AR/NIAMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources