

Economic impact of the clinical benefits of bariatric surgery in diabetes patients with BMI ≥35 kg/m²
- PMID: 20829800
- PMCID: PMC3721344
- DOI: 10.1038/oby.2010.199
Economic impact of the clinical benefits of bariatric surgery in diabetes patients with BMI ≥35 kg/m²
Abstract
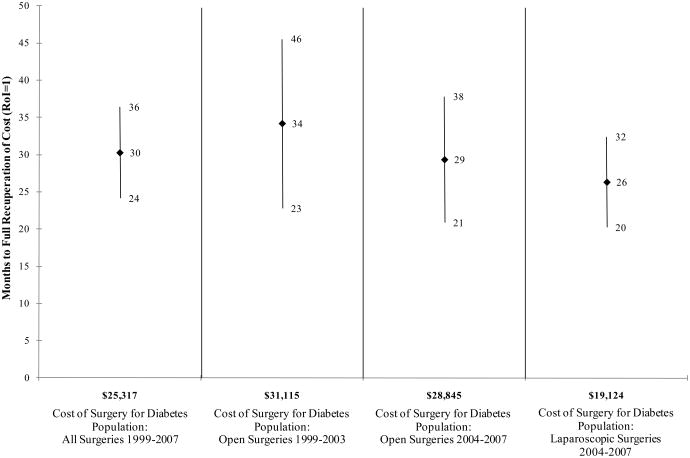
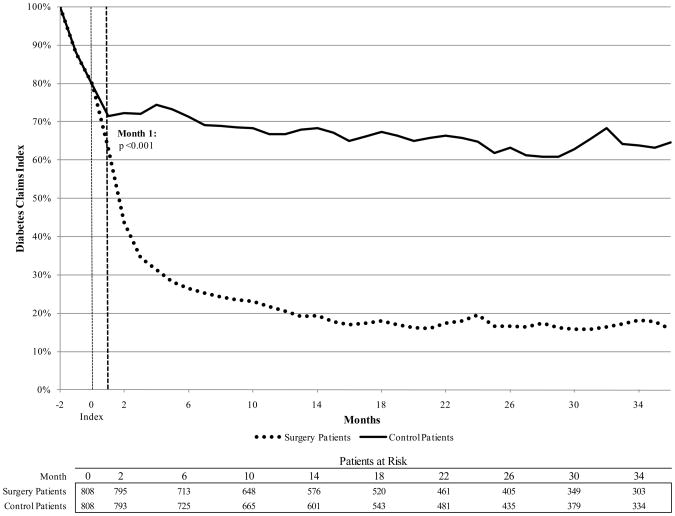
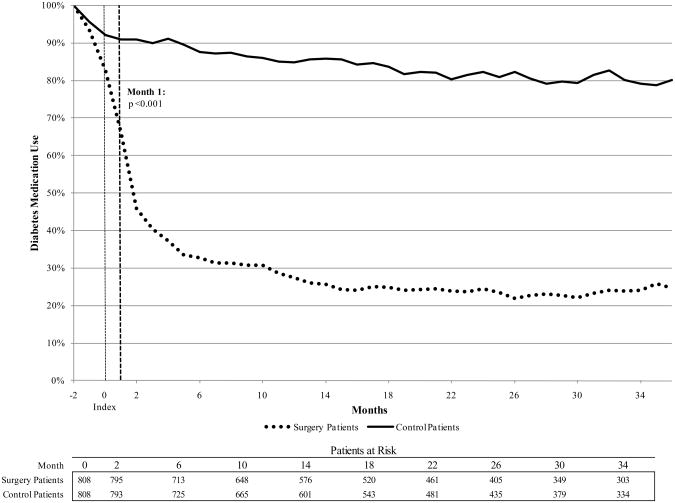
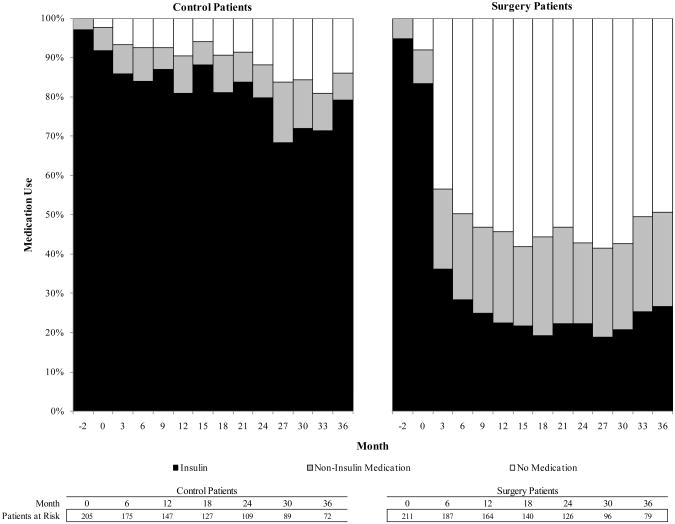
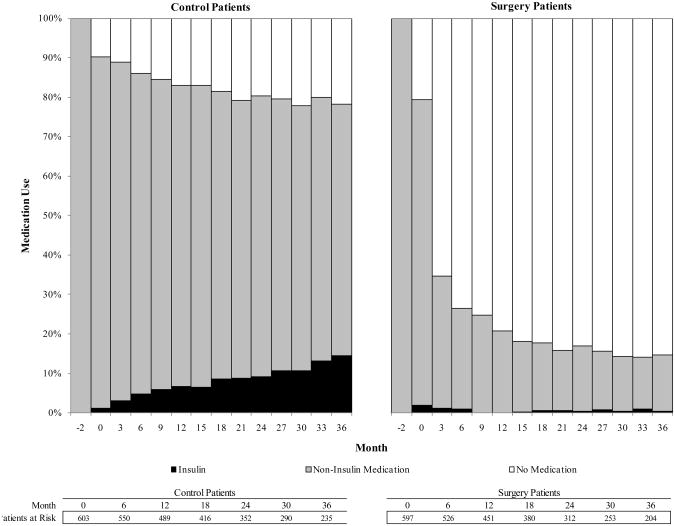
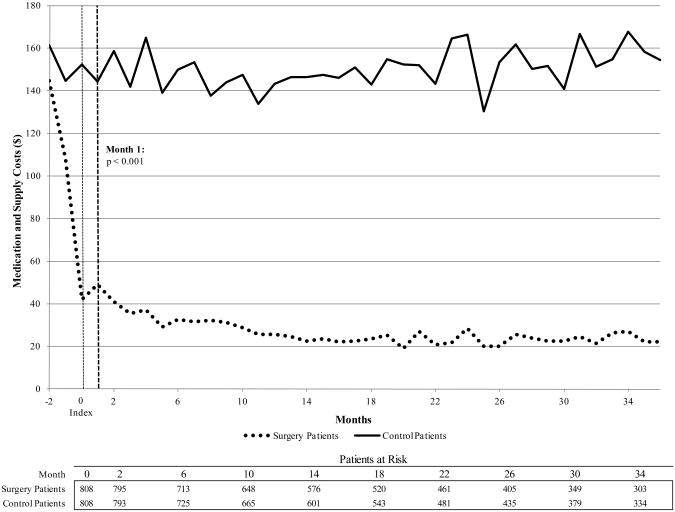
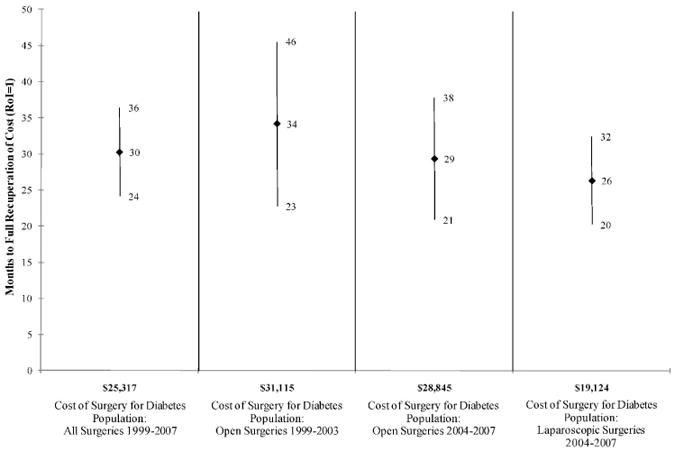
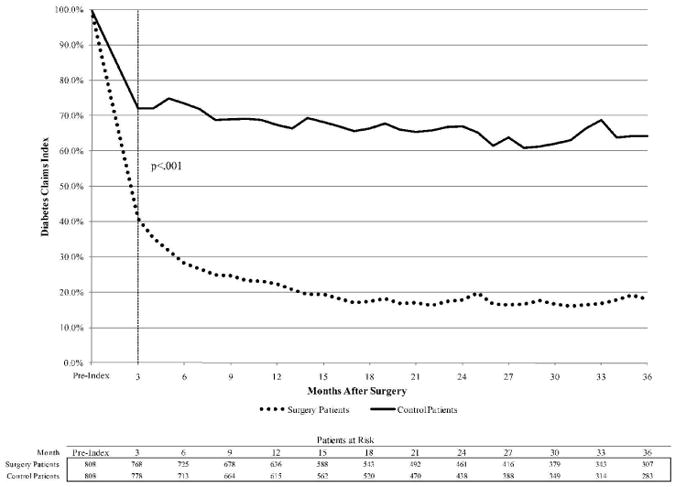
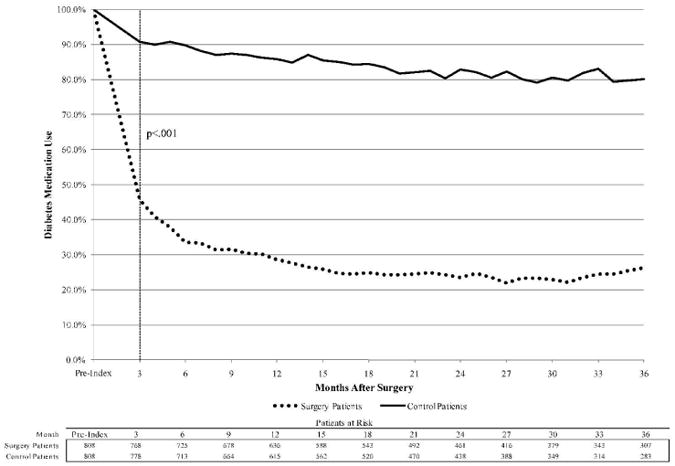
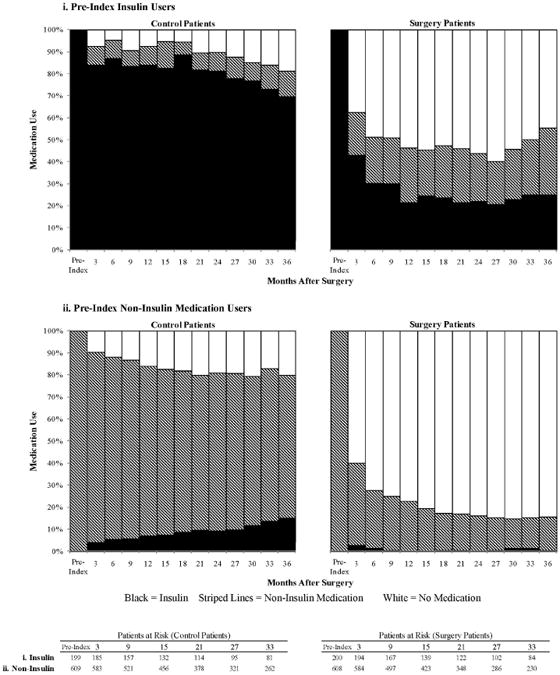
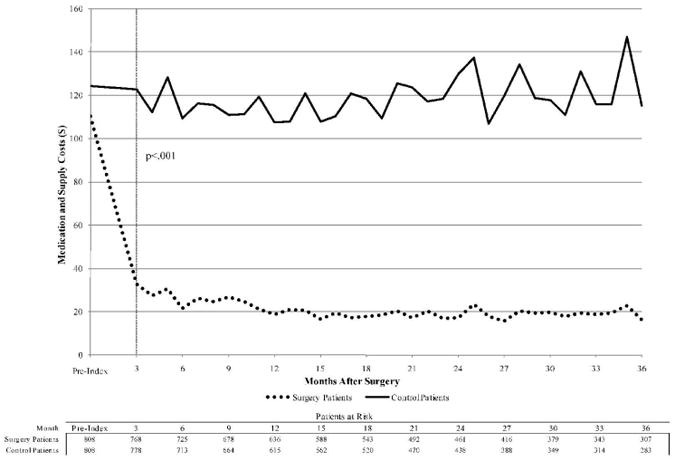
The medical costs for a type 2 diabetes patient are two to four times greater than the costs for a patient without diabetes. Bariatric surgery is the most effective weight-loss therapy and has marked therapeutic effects on diabetes. We estimate the economic effect of the clinical benefits of bariatric surgery for diabetes patients with BMI ≥ 35 kg/m². Using an administrative claims database of privately insured patients covering 8.5 million lives 1999-2007, we identify obese patients with diabetes, aged 18-65 years, who were treated with bariatric surgery identified using Healthcare Common Procedure Coding System codes. These patients were matched with nonsurgery control patients on demographic factors, comorbidities, and health-care costs. The overall return on investment (RoI) associated with bariatric surgery was calculated using multivariate analysis. Surgery and control patients were compared postindex with respect to diagnostic claims for diabetes, diabetes medication claims, and adjusted diabetes medication and supply costs. Surgery costs were fully recovered after 26 months for laparoscopic surgery. At month 6, 28% of surgery patients had a diabetes diagnosis, compared to 74% of control patients (P < 0.001). Among preindex insulin users, insulin use dropped to 43% by month 3 for surgery patients, vs. 84% for controls (P < 0.001). By month 1, medication and supply costs were significantly lower for surgery patients (P < 0.001). The therapeutic benefits of bariatric surgery on diabetes translate into considerable economic benefits. These data suggest that surgical therapy is clinically more effective and ultimately less expensive than standard therapy for diabetes patients with BMI ≥ 35 kg/m².
Figures
References
-
- National diabetes fact sheet: United States, 2007. CDC Diabetes. 2007
-
- Campbell RK, Martin TM. The chronic burden of diabetes. Am J Manag Care. 2009;15:S248–S254. - PubMed
-
- Ford ES, Williamson DF, Liu S. Weight changes and diabetes incidence: findings from a national cohort of US adults. Am J Epidemiology. 1997;146:214–222. - PubMed
-
- Colditz GA, Willett WC, Rotnitzky A, Manson JE. Weight gain as a risk factor for clinical diabetes mellitus in women. Ann Intern Med. 1995;122:481–486. - PubMed
-
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and trends in obesity among US adults. [Accessed June 12,2007. Accessed August 21, 2008];JAMA. 2010 Jan 13; published online. http://www.niddk.nih.gov/health/nutrit/pubs/statobes.htm. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
