

A mouse model of post-arthroplasty Staphylococcus aureus joint infection to evaluate in vivo the efficacy of antimicrobial implant coatings
- PMID: 20830204
- PMCID: PMC2935351
- DOI: 10.1371/journal.pone.0012580
A mouse model of post-arthroplasty Staphylococcus aureus joint infection to evaluate in vivo the efficacy of antimicrobial implant coatings
Abstract
Background: Post-arthroplasty infections represent a devastating complication of total joint replacement surgery, resulting in multiple reoperations, prolonged antibiotic use, extended disability and worse clinical outcomes. As the number of arthroplasties in the U.S. will exceed 3.8 million surgeries per year by 2030, the number of post-arthroplasty infections is projected to increase to over 266,000 infections annually. The treatment of these infections will exhaust healthcare resources and dramatically increase medical costs.
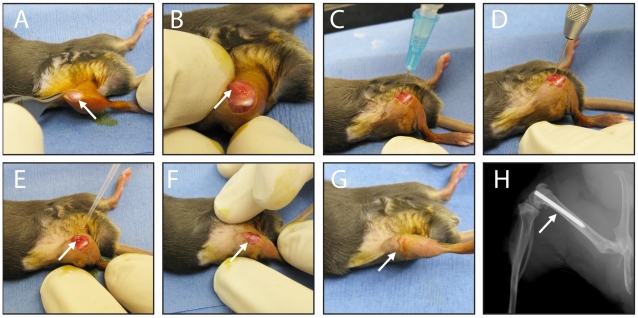
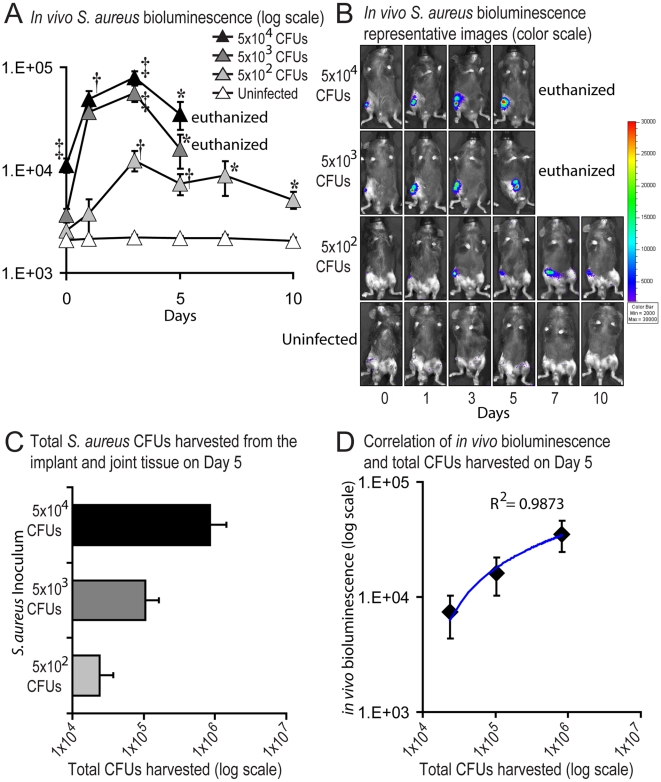
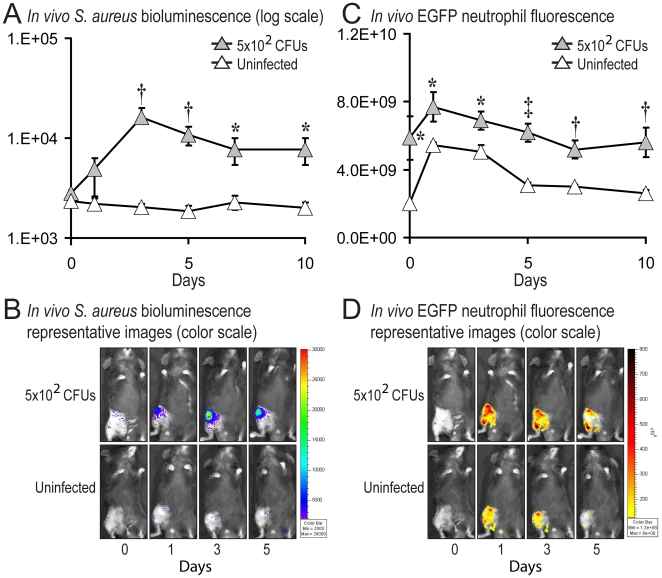
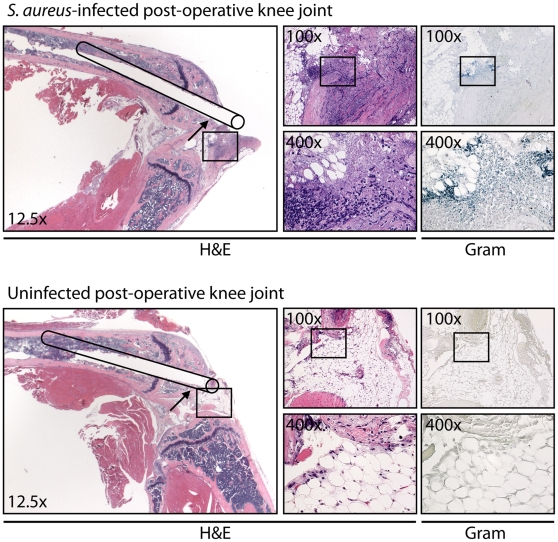
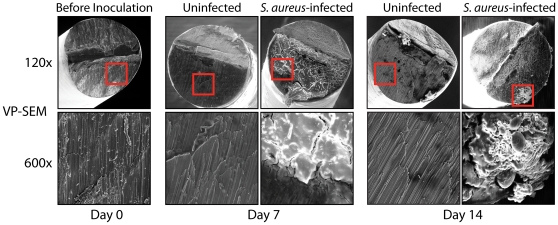
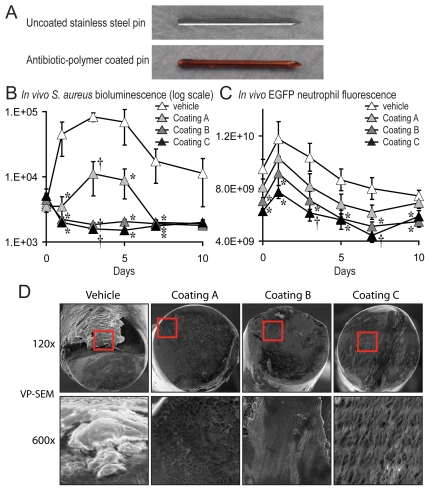
Methodology/principal findings: To evaluate novel preventative therapeutic strategies against post-arthroplasty infections, a mouse model was developed in which a bioluminescent Staphylococcus aureus strain was inoculated into a knee joint containing an orthopaedic implant and advanced in vivo imaging was used to measure the bacterial burden in real-time. Mice inoculated with 5x10(3) and 5x10(4) CFUs developed increased bacterial counts with marked swelling of the affected leg, consistent with an acute joint infection. In contrast, mice inoculated with 5x10(2) CFUs developed a low-grade infection, resembling a more chronic infection. Ex vivo bacterial counts highly correlated with in vivo bioluminescence signals and EGFP-neutrophil fluorescence of LysEGFP mice was used to measure the infection-induced inflammation. Furthermore, biofilm formation on the implants was visualized at 7 and 14 postoperative days by variable-pressure scanning electron microscopy (VP-SEM). Using this model, a minocycline/rifampin-impregnated bioresorbable polymer implant coating was effective in reducing the infection, decreasing inflammation and preventing biofilm formation.
Conclusions/significance: Taken together, this mouse model may represent an alternative pre-clinical screening tool to evaluate novel in vivo therapeutic strategies before studies in larger animals and in human subjects. Furthermore, the antibiotic-polymer implant coating evaluated in this study was clinically effective, suggesting the potential for this strategy as a therapeutic intervention to combat post-arthroplasty infections.
Conflict of interest statement
Figures
References
-
- Kurtz SM, Lau E, Schmier J, Ong KL, Zhao K, et al. Infection burden for hip and knee arthroplasty in the United States. J Arthroplasty. 2008;23:984–991. - PubMed
-
- Bozic KJ, Ries MD. The impact of infection after total hip arthroplasty on hospital and surgeon resource utilization. J Bone Joint Surg Am. 2005;87:1746–1751. - PubMed
-
- Urquhart DM, Hanna FS, Brennan SL, Wluka AE, Leder K, et al. Incidence and Risk Factors for Deep Surgical Site Infection After Primary Total Hip Arthroplasty: A Systematic Review. J Arthroplasty. 2009 S0883-5403(09)00411-2 [pii];10.1016/j.arth.2009.08.011 [doi] - PubMed
-
- Bozic KJ, Kurtz SM, Lau E, Ong K, Vail TP, et al. The epidemiology of revision total hip arthroplasty in the United States. J Bone Joint Surg Am. 2009;91:128–133. 91/1/128 [pii];10.2106/JBJS.H.00155 [doi] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
