

Medicaid and preterm births in Virginia: an analysis of recent outcomes
- PMID: 20831442
- PMCID: PMC2971635
- DOI: 10.1089/jwh.2010.1955
Medicaid and preterm births in Virginia: an analysis of recent outcomes
Abstract
Objectives: The study objectives were to evaluate adequacy of prenatal care and risk for preterm birth among Medicaid clients in Virginia and to determine if payment method is associated with the risk of preterm birth.
Methods: Birth certificate data for the Commonwealth of Virginia for 2007 and 2008 were linked with Medicaid claims data. Analysis was limited to singleton births. Three payment methods were evaluated: private insurance, self-pay, and Medicaid. The prevalence of preterm birth for each level of prenatal care defined by the Kotelchuck prenatal care index was assessed for each payment method. Unconditional logistic regression modeling was used to assess the association between payment method and preterm birth risk while controlling for known preterm birth risk factors.
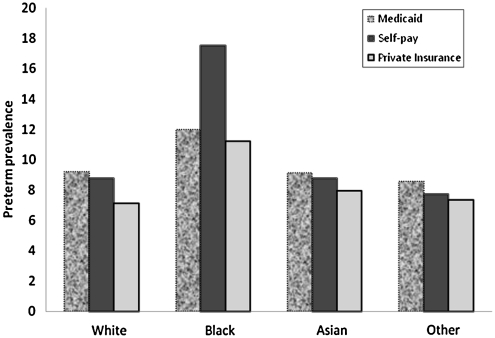
Results: Preterm birth prevalences (95% confidence interval [CI]) for the different payment methods were 7.9% (4.79-8.07) for the privately insured, 10.1% (9.57-10.60) for the self-pay group, and 10.2% (9.95-10.45) for Medicaid recipients. Compared with those with private insurance, women on Medicaid had an adjusted odds ratio (OR) for preterm birth (95% CI) of 0.99 (0.94-1.03). Self-pay mothers had a 32% increase in the odds of preterm birth relative to the privately insured. All payment groups show a trend toward significant reduction in preterm birth prevalence as adequacy of prenatal care improved from inadequate to adequate. Medicaid enrollees had a high prevalence of known risk factors, including smoking and illicit drug use and cervical insufficiency.
Conclusions: When known risk factors have been controlled, preterm birth risk for Medicaid enrollees did not differ significantly from the privately insured.
Figures
Similar articles
-
Association of the Affordable Care Act Dependent Coverage Provision With Prenatal Care Use and Birth Outcomes.JAMA. 2018 Feb 13;319(6):579-587. doi: 10.1001/jama.2018.0030. JAMA. 2018. PMID: 29450525 Free PMC article.
-
Medicaid and preterm birth and low birth weight: the last two decades.J Womens Health (Larchmt). 2010 Mar;19(3):443-51. doi: 10.1089/jwh.2009.1602. J Womens Health (Larchmt). 2010. PMID: 20141370 Free PMC article. Review.
-
An Analysis of Payment Mix Patterns of Preterm Births in a Post-Affordable Care Act Insurance Market: Implications for the Medicaid Program.Womens Health Issues. 2020 Jul-Aug;30(4):248-259. doi: 10.1016/j.whi.2020.04.003. Epub 2020 Jun 4. Womens Health Issues. 2020. PMID: 32505430
-
Source of payment for the delivery: births in a 33-state and District of Columbia reporting area, 2010.Natl Vital Stat Rep. 2013 Dec 19;62(5):1-20. Natl Vital Stat Rep. 2013. PMID: 24364892
-
Preterm delivery and psycho-social determinants of health based on World Health Organization model in Iran: a narrative review.Glob J Health Sci. 2012 Nov 4;5(1):52-64. doi: 10.5539/gjhs.v5n1p52. Glob J Health Sci. 2012. PMID: 23283036 Free PMC article. Review.
Cited by
-
Patient-, Hospital-, and Neighborhood-Level Factors Associated with Severe Maternal Morbidity During Childbirth: A Cross-Sectional Study in New York State 2013-2014.Matern Child Health J. 2019 Jan;23(1):82-91. doi: 10.1007/s10995-018-2596-9. Matern Child Health J. 2019. PMID: 30014373
-
Racial disparities in economic and clinical outcomes of pregnancy among Medicaid recipients.Matern Child Health J. 2013 Oct;17(8):1518-25. doi: 10.1007/s10995-012-1162-0. Matern Child Health J. 2013. PMID: 23065298 Free PMC article.
-
A comparison of approaches to identify live births using the medicaid analytic extract.Health Serv Outcomes Res Methodol. 2022 Mar;22(1):49-58. doi: 10.1007/s10742-021-00252-w. Epub 2021 May 26. Health Serv Outcomes Res Methodol. 2022. PMID: 35463943 Free PMC article.
-
Characterizing Hypertensive Disorders of Pregnancy Among Medicaid Recipients in a Nonexpansion State.J Womens Health (Larchmt). 2022 Feb;31(2):261-269. doi: 10.1089/jwh.2020.8741. Epub 2021 Jun 10. J Womens Health (Larchmt). 2022. PMID: 34115529 Free PMC article.
-
Prospective longitudinal study of the pregnancy DNA methylome: the US Pregnancy, Race, Environment, Genes (PREG) study.BMJ Open. 2018 May 9;8(5):e019721. doi: 10.1136/bmjopen-2017-019721. BMJ Open. 2018. PMID: 29743320 Free PMC article.
References
-
- Mathews TJ. MacDorman MF. National vital statistics reports. 2. Vol. 57. Hyattsville, MD: National Center for Health Statistics; 2008. Infant mortality statistics from the 2005 period linked birth/infant death data set. - PubMed
-
- Rosenbaum S. Medicaid and national health care reform. N Engl J Med. 2009;361:2009–2012. - PubMed
-
- Adams EK. Gavin NI. Handler A. Manning W. Raskind-Hood C. Transitions in insurance coverage from before pregnancy through delivery in nine states, 1996–1999. Health Aff (Millwood) 2003;22:219–229. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
