

Feasibility and sensitivity study of helical tomotherapy for dose painting plans
- PMID: 20831487
- PMCID: PMC3040036
- DOI: 10.3109/0284186X.2010.500302
Feasibility and sensitivity study of helical tomotherapy for dose painting plans
Abstract
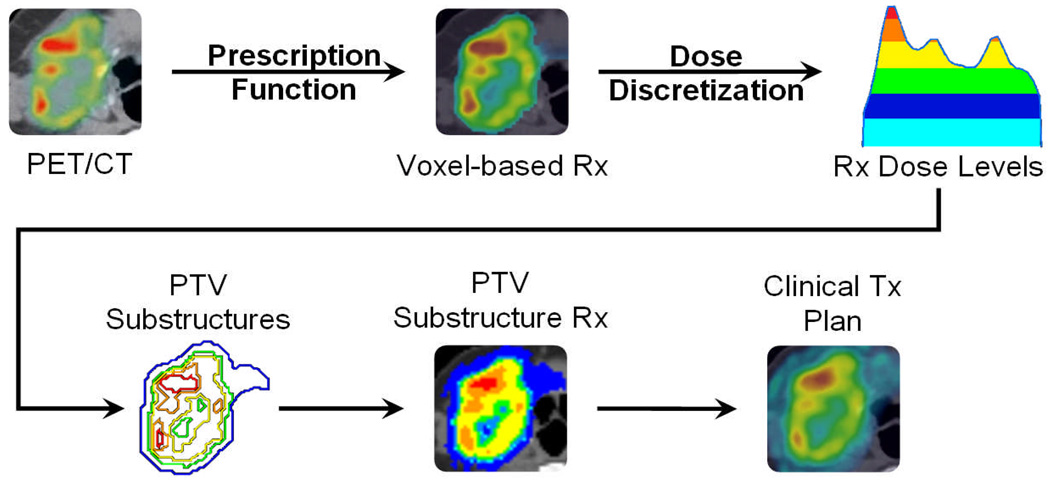
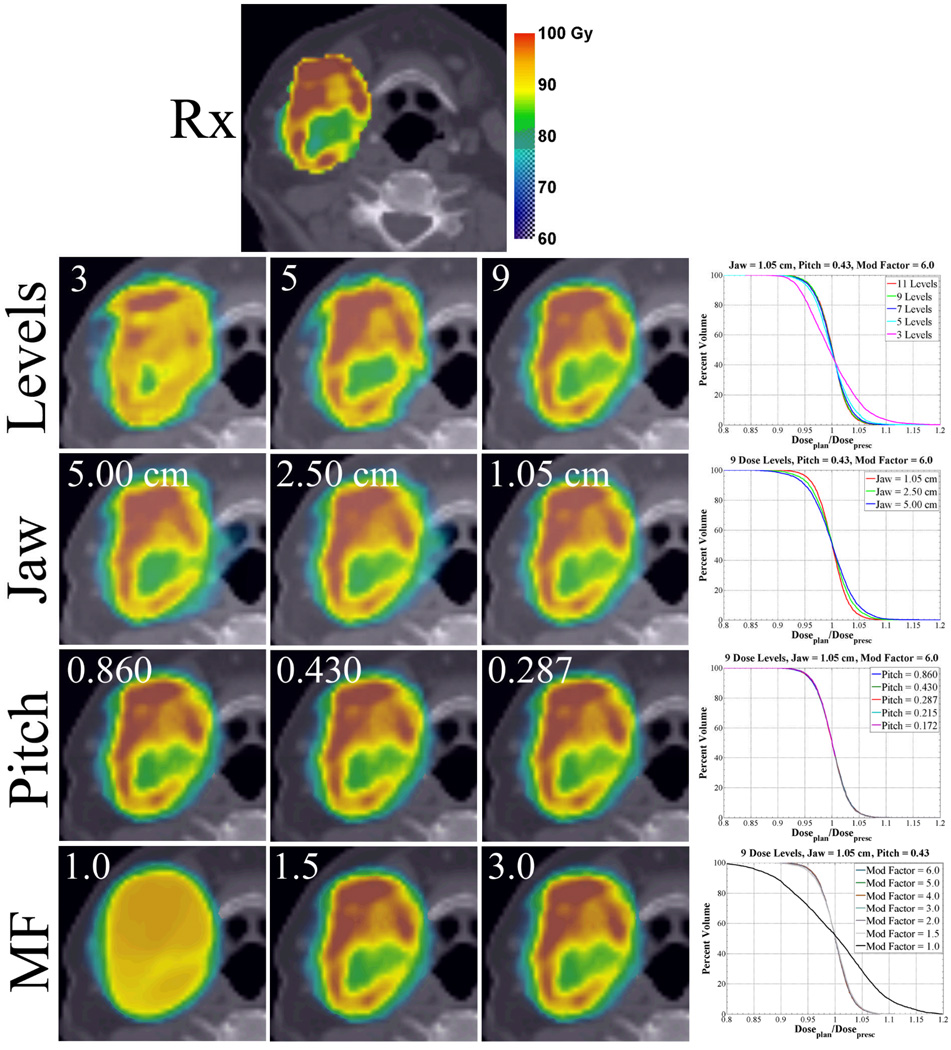
Important limitations for dose painting are due to treatment planning and delivery constraints. The purpose of this study was to develop a methodology for creating voxel-based dose painting plans that are deliverable using the clinical TomoTherapy Hi-Art II treatment planning system (TPS). Material and methods. Uptake data from a head and neck patient who underwent a [(61)Cu]Cu-ATSM (hypoxia surrogate) PET/CT scan was retrospectively extracted for planning. Non-uniform voxel-based prescriptions were converted to structured-based prescriptions for compatibility with the Hi-Art II TPS. Optimized plans were generated by varying parameters such as dose level, structure importance, prescription point normalization, DVH volume, min/max dose, and dose penalty. Delivery parameters such as pitch, jaw width and modulation factor were also varied. Isodose distributions, quality volume histograms and planning target volume percentage receiving planned dose within 5% of the prescription (Q(0.95-1.05)) were used to evaluate plan conformity. Results. In general, the conformity of treatment plans to dose prescriptions was found to be adequate for delivery of dose painting plans. The conformity was better as the dose levels increased from three to nine levels (Q(0.95-1.05): 69% to 93%), jaw decreased in width from 5.0cm to 1.05cm (Q(0.95-1.05): 81% to 93%), and modulation factor increased up to 2.0 (Q(0.95-1.05): 36% to 92%). The conformity was invariant to changes in pitch. Plan conformity decreased as the prescription DVH constraint (Q(0.95-1.05): 93% vs. 89%) or the normalization point (Q(0.95-1.05): 93% vs. 90%) deviated from the means. Conclusion. This investigation demonstrated the ability of the Hi-Art II TPS to create voxel-based dose painting plans. Results indicated that agreement in prescription dose and planned dose distributions for all plans were sensitive to physical delivery parameter changes in jaw width and modulation factors, but insensitive to changes in pitch. Tight constraints on target structures also resulted in decreased plan conformity while under a relaxed set of optimization parameters, plan conformity was increased.
Figures
References
-
- Chao KS, Perez CA, Brady LW. Radiation Oncology: management decisions. 2nd ed. Philadeplphia: Lippincott Williams & Wilkins; 2002. p. xi.
-
- Chao KS, Ozyigit G, Tran BN, Cengiz M, Dempsey JF, Low DA. Patterns of failure in patients receiving definitive and postoperative IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2003;55(2):312–321. - PubMed
-
- Pucar D, Hricak H, Shukla-Dave A, Kuroiwa K, Drobnjak M, Eastham J, et al. Clinically significant prostate cancer local recurrence after radiation therapy occurs at the site of primary tumor: magnetic resonance imaging and step-section pathology evidence. Int J Radiat Oncol Biol Phys. 2007;69(1):62–69. - PubMed
-
- Lauve AM, Morris M, Schmidt-Ullrich R, Wu Q, Mohan O, Abayomi D, et al. Simultaneous integrated boost intensity-modulated radiotherapy for locally advanced head-and-neck squamous cell carcinomas: II—clinical results. Int J Radiat Oncol Biol Phys. 2004;60(2):374–387. - PubMed
-
- Ling CC, Humm J, Larson S, Amols H, Fuks Z, Leibel S, et al. Towards multidimensional radiotherapy (MD-CRT): biological imaging and biological conformality. Int J Radiat Oncol Biol Phys. 2000;47(3):551–560. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical