

Normal Tissue Complication Probability (NTCP) modeling of late rectal bleeding following external beam radiotherapy for prostate cancer: A Test of the QUANTEC-recommended NTCP model
- PMID: 20831493
- PMCID: PMC4786007
- DOI: 10.3109/0284186X.2010.509736
Normal Tissue Complication Probability (NTCP) modeling of late rectal bleeding following external beam radiotherapy for prostate cancer: A Test of the QUANTEC-recommended NTCP model
Abstract
Purpose/background: Validating a predictive model for late rectal bleeding following external beam treatment for prostate cancer would enable safer treatments or dose escalation. We tested the normal tissue complication probability (NTCP) model recommended in the recent QUANTEC review (quantitative analysis of normal tissue effects in the clinic).
Material and methods: One hundred and sixty one prostate cancer patients were treated with 3D conformal radiotherapy for prostate cancer at the British Columbia Cancer Agency in a prospective protocol. The total prescription dose for all patients was 74 Gy, delivered in 2 Gy/fraction. 159 3D treatment planning datasets were available for analysis. Rectal dose volume histograms were extracted and fitted to a Lyman-Kutcher-Burman NTCP model.
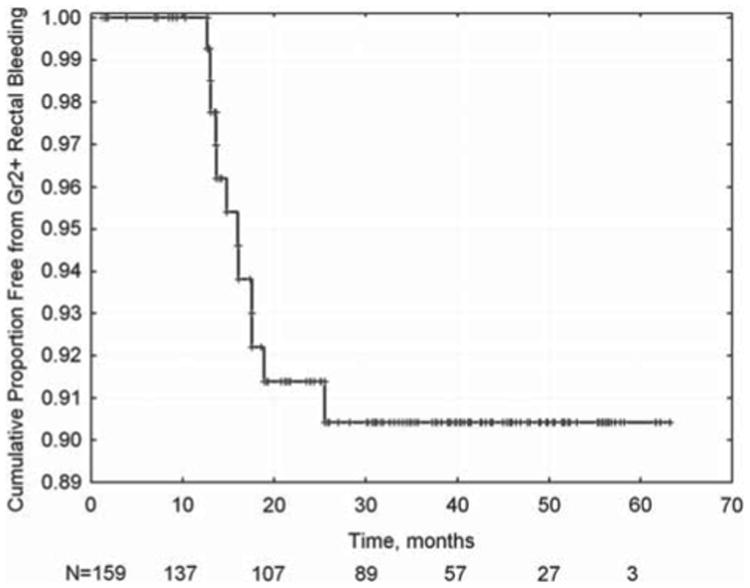
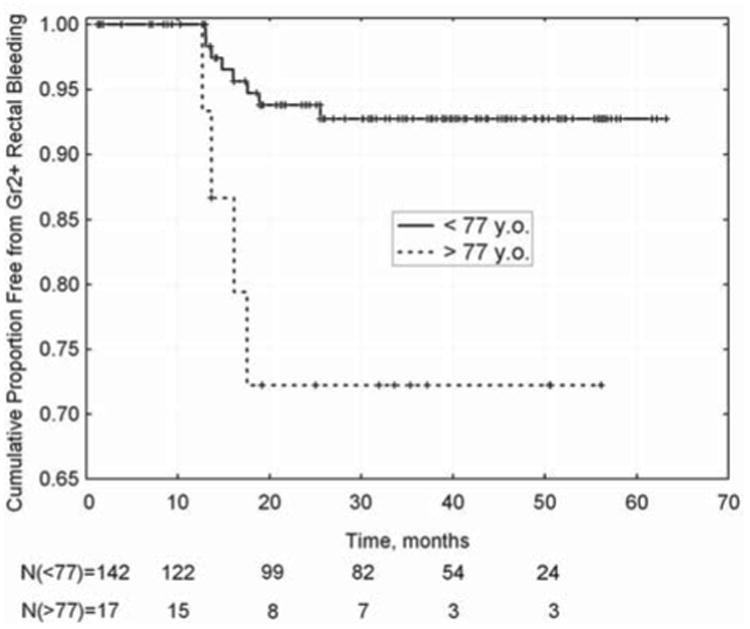
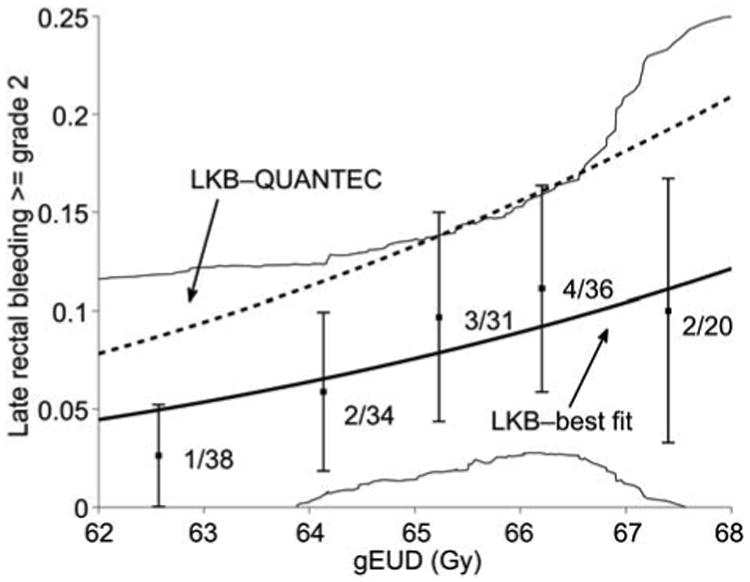
Results: Late rectal bleeding (>grade 2) was observed in 12/159 patients (7.5%). Multivariate logistic regression with dose-volume parameters (V50, V60, V70, etc.) was non-significant. Among clinical variables, only age was significant on a Kaplan-Meier log-rank test (p=0.007, with an optimal cut point of 77 years). Best-fit Lyman-Kutcher-Burman model parameters (with 95% confidence intervals) were: n = 0.068 (0.01, +infinity); m =0.14 (0.0, 0.86); and TD50 = 81 (27, 136) Gy. The peak values fall within the 95% QUANTEC confidence intervals. On this dataset, both models had only modest ability to predict complications: the best-fit model had a Spearman's rank correlation coefficient of rs = 0.099 (p = 0.11) and area under the receiver operating characteristic curve (AUC) of 0.62; the QUANTEC model had rs=0.096 (p= 0.11) and a corresponding AUC of 0.61. Although the QUANTEC model consistently predicted higher NTCP values, it could not be rejected according to the χ(2) test (p = 0.44).
Conclusions: Observed complications, and best-fit parameter estimates, were consistent with the QUANTEC-preferred NTCP model. However, predictive power was low, at least partly because the rectal dose distribution characteristics do not vary greatly within this patient cohort.
Conflict of interest statement
Figures
Similar articles
-
Prediction of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer.Radiat Oncol. 2015 Apr 8;10:80. doi: 10.1186/s13014-015-0389-5. Radiat Oncol. 2015. PMID: 25890376 Free PMC article.
-
Fitting late rectal bleeding data using different NTCP models: results from an Italian multi-centric study (AIROPROS0101).Radiother Oncol. 2004 Oct;73(1):21-32. doi: 10.1016/j.radonc.2004.08.013. Radiother Oncol. 2004. PMID: 15465142
-
Random forests to predict rectal toxicity following prostate cancer radiation therapy.Int J Radiat Oncol Biol Phys. 2014 Aug 1;89(5):1024-1031. doi: 10.1016/j.ijrobp.2014.04.027. Epub 2014 Jul 8. Int J Radiat Oncol Biol Phys. 2014. PMID: 25035205 Clinical Trial.
-
Dose-volume analysis of predictors for chronic rectal toxicity after treatment of prostate cancer with adaptive image-guided radiotherapy.Int J Radiat Oncol Biol Phys. 2005 Aug 1;62(5):1297-308. doi: 10.1016/j.ijrobp.2004.12.052. Int J Radiat Oncol Biol Phys. 2005. PMID: 16029785 Review.
-
Radiation dose-volume effects in radiation-induced rectal injury.Int J Radiat Oncol Biol Phys. 2010 Mar 1;76(3 Suppl):S123-9. doi: 10.1016/j.ijrobp.2009.03.078. Int J Radiat Oncol Biol Phys. 2010. PMID: 20171506 Free PMC article. Review.
Cited by
-
Dependence of the safe rectum dose on the CTV-PTV margin size and treatment technique.Rep Pract Oncol Radiother. 2015 May-Jun;20(3):198-203. doi: 10.1016/j.rpor.2014.12.004. Epub 2015 Jan 7. Rep Pract Oncol Radiother. 2015. PMID: 25949223 Free PMC article.
-
Prediction of gastrointestinal toxicity after external beam radiotherapy for localized prostate cancer.Radiat Oncol. 2015 Apr 8;10:80. doi: 10.1186/s13014-015-0389-5. Radiat Oncol. 2015. PMID: 25890376 Free PMC article.
-
Image-guided radiotherapy of the prostate using daily CBCT: the feasibility and likely benefit of implementing a margin reduction.Br J Radiol. 2014 Dec;87(1044):20140459. doi: 10.1259/bjr.20140459. Epub 2014 Oct 29. Br J Radiol. 2014. PMID: 25354015 Free PMC article. Clinical Trial.
-
Evaluating the Predictive Value of the Dose-volume Parameters and Vascular Endothelial Growth Factor Expression on Rectal Toxicity in Prostate Cancer Patients.J Med Phys. 2024 Oct-Dec;49(4):539-544. doi: 10.4103/jmp.jmp_67_24. Epub 2024 Dec 18. J Med Phys. 2024. PMID: 39926150 Free PMC article.
-
A Systematic Post-QUANTEC Review of Tolerance Doses for Late Toxicity After Prostate Cancer Radiation Therapy.Int J Radiat Oncol Biol Phys. 2018 Dec 1;102(5):1514-1532. doi: 10.1016/j.ijrobp.2018.08.015. Epub 2018 Aug 17. Int J Radiat Oncol Biol Phys. 2018. PMID: 30125635 Free PMC article.
References
-
- Bentzen SM. From cellular to high-throughput predictive assays in radiation oncology: Challenges and opportunities. Semin Radiat Oncol. 2008;18:75–88. - PubMed
-
- Deasy JO, Blanco AI, Clark VH. CERR: A Computational Environment for Radiotherapy Research. Med Phys. 2003;30:979–85. - PubMed
-
- Peeters ST, Lebesque JV, Heemsbergen WD, van Putten WL, Slot A, Dielwart MF, Koper PC. Localized volume effects for late rectal and anal toxicity after radiotherapy for prostate cancer. Int J Radiat Oncol Biol Phys. 2006;64:1151–61. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical