

The optimum follow-up period for assessing mortality outcomes in injured older adults
- PMID: 20831727
- PMCID: PMC2952068
- DOI: 10.1111/j.1532-5415.2010.03065.x
The optimum follow-up period for assessing mortality outcomes in injured older adults
Abstract
Objectives: To compare mortality rates of hospitalized injured aged 67 and older across commonly used follow-up periods (e.g., in-hospital, 30-day, 1-year) and to determine the postinjury time after which mortality rates stabilize.
Design: Retrospective analysis of Medicare claims.
Setting: Oregon and Washington Medicare patients.
Participants: Patients admitted to 171 Oregon and Washington facilities during 2001/02 with injuries identified according to International Classification of Diseases, Ninth Revision, code and followed for 1 year.
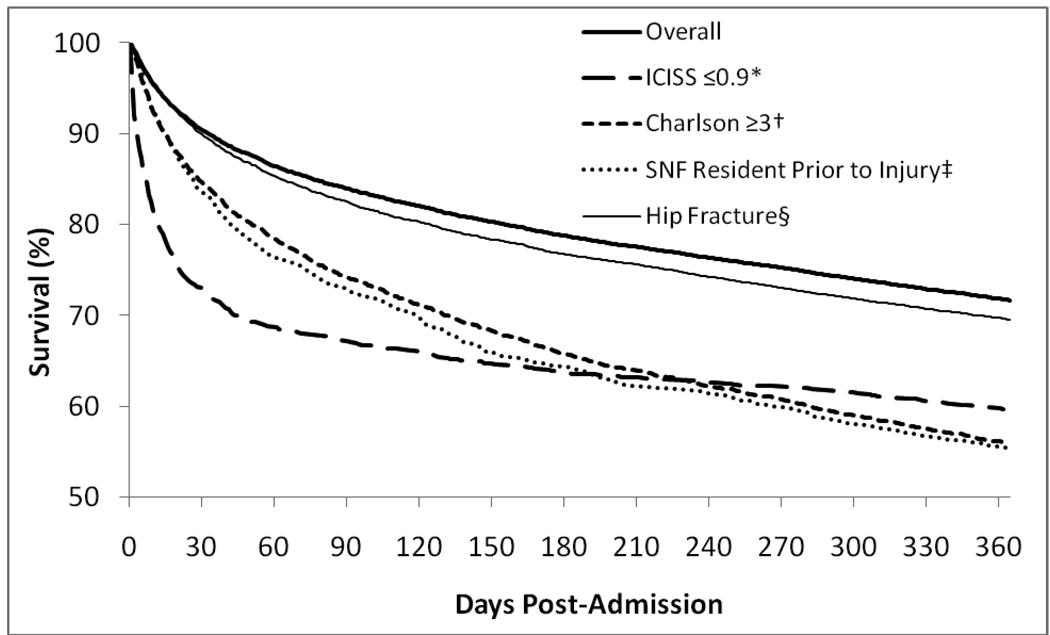
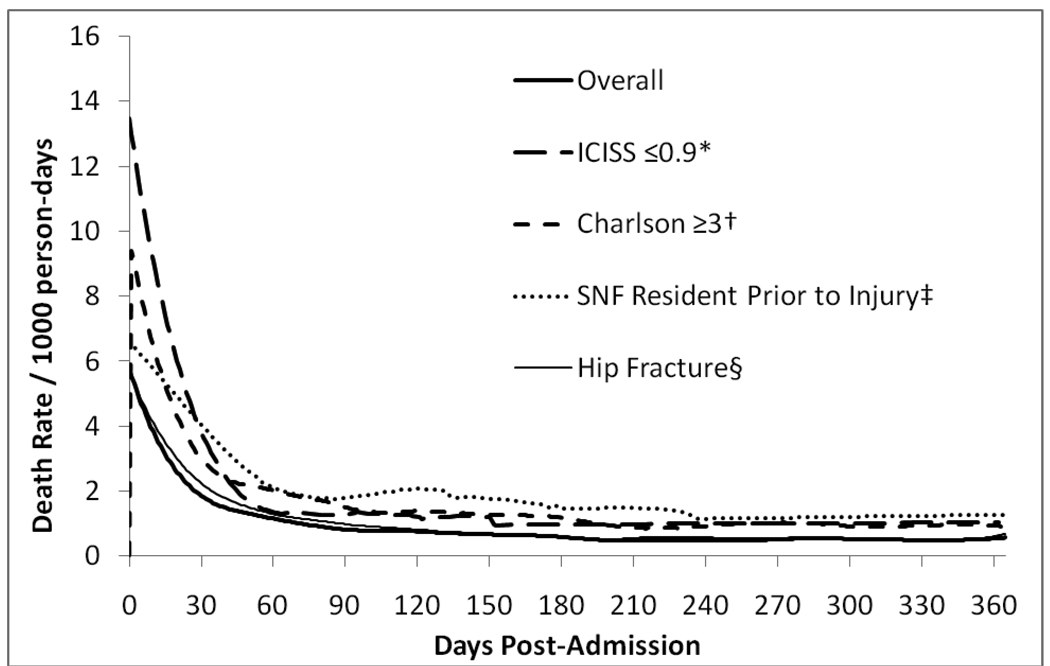
Measurements: The primary outcome was in-hospital mortality and mortality at 30, 60, 90, 180, and 365 days. Kaplan-Meier survival curves and daily postadmission mortality rates were also evaluated. The rate of change (slope) of the survival curves and daily mortality rates were analyzed to select the point after which mortality rates were no longer decreasing.
Results: There were 32,135 injured older adults hospitalized over the 2-year period, with a median age of 82 (interquartile range 77-88). Cumulative in-hospital mortality and at 30, 60, 90, 180, and 365 days was 4.1%, 9.7%, 13.6%, 16.1%, 21.3%, and 28.4%, respectively. Mortality rates stabilized by 6 months after injury, with 89% of the change occurring within 60 days. Although serious injuries, medical comorbidities, and preinjury nursing facility residence were all associated with higher mortality, they did not affect the pattern of mortality after injury.
Conclusion: In-hospital mortality is much lower than postdischarge mortality in injured older adults, with a substantial portion of persons dying shortly after discharge from the hospital. Mortality appears to stabilize by 6 months after injury, although 60-day postadmission follow-up captures most of the excess daily mortality rate.
© 2010, Copyright the Authors. Journal compilation © 2010, The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Gubler KD, Davis R, Koepsell T, et al. Long-term survival of elderly trauma patients. Arch Surg. 1997;132:1010–1014. - PubMed
-
- McGwin G, Melton SM, May AK, et al. Long-term survival in the elderly after trauma. J Trauma. 2000;49:470–476. - PubMed
-
- Clark DE, DeLorenzo MA, Lucas FL, et al. Epidemiology and short-term outcomes of injured medicare patients. J Am Geriatr Soc. 2004;52:2023–2030. - PubMed
-
- Shyu YI, Liang J, Wu C, et al. Interdisciplinary Intervention for Hip Fracture in Older Taiwanese: Benefits Last for 1 Year. J Gerontol. 2008;63:92–97. - PubMed
-
- Mullins RJ, Mann NC, Hedges JR, et al. Adequacy of hospital discharge status as a measure of outcome among injured patients. JAMA. 1998;279:1727–1731. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
