

Routine resite of peripheral intravenous devices every 3 days did not reduce complications compared with clinically indicated resite: a randomised controlled trial
- PMID: 20831782
- PMCID: PMC2944158
- DOI: 10.1186/1741-7015-8-53
Routine resite of peripheral intravenous devices every 3 days did not reduce complications compared with clinically indicated resite: a randomised controlled trial
Abstract
Background: Peripheral intravenous device (IVD) complications were traditionally thought to be reduced by limiting dwell time. Current recommendations are to resite IVDs by 96 hours with the exception of children and patients with poor veins. Recent evidence suggests routine resite is unnecessary, at least if devices are inserted by a specialised IV team. The aim of this study was to compare the impact of peripheral IVD 'routine resite' with 'removal on clinical indication' on IVD complications in a general hospital without an IV team.
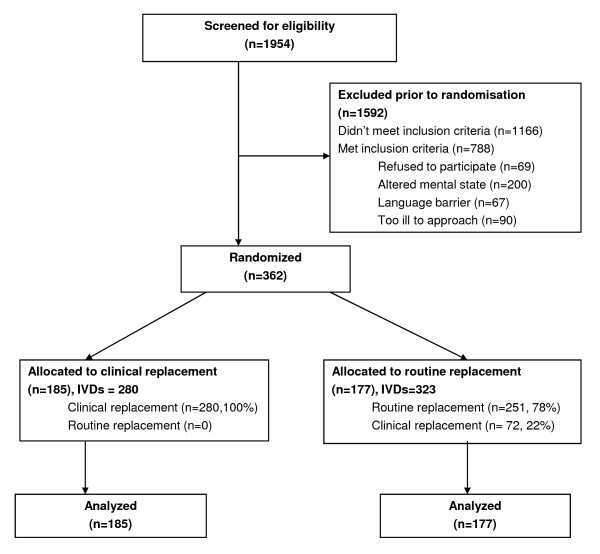
Methods: A randomised, controlled trial was conducted in a regional teaching hospital. After ethics approval, 362 patients (603 IVDs) were randomised to have IVDs replaced on clinical indication (185 patients) or routine change every 3 days (177 patients). IVDs were inserted and managed by the general hospital medical and nursing staff; there was no IV team. The primary endpoint was a composite of IVD complications: phlebitis, infiltration, occlusion, accidental removal, local infection, and device-related bloodstream infection.
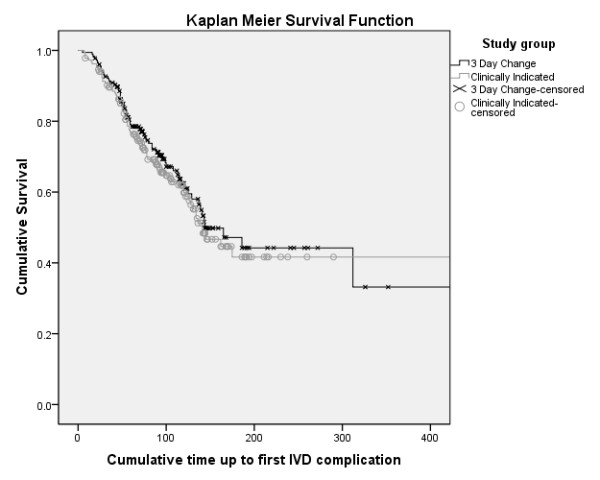
Results: IVD complication rates were 68 per 1,000 IVD days (clinically indicated) and 66 per 1,000 IVD days (routine replacement) (P = 0.86; HR 1.03; 95% CI, 0.74-1.43). Time to first complication per patient did not differ between groups (KM with log rank, P = 0.53). There were no local infections or IVD-related bloodstream infections in either group. IV therapy duration did not differ between groups (P = 0.22), but more (P = 0.004) IVDs were placed per patient in the routine replacement (mean, 1.8) than the clinical indication group (mean, 1.5), with significantly higher hospital costs per patient (P < 0.001).
Conclusions: Resite on clinical indication would allow one in two patients to have a single cannula per course of IV treatment, as opposed to one in five patients managed with routine resite; overall complication rates appear similar. Clinically indicated resite would achieve savings in equipment, staff time and patient discomfort. There is growing evidence to support the extended use of peripheral IVDs with removal only on clinical indication.
Registration number: Australian New Zealand Clinical Trials Registry (ANZCTR) Number ACTRN12608000421336.
Figures
References
-
- Maki DG, Ringer M. Risk factors for infusion-related phlebitis with small peripheral venous catheters. Ann Intern Med. 1991;114(10):845–854. - PubMed
-
- Monreal M, Oller B, Rodriguez N, Vega J, Torres T, Valero P, Mach G, Ruiz AE, Roca J. Infusion phlebitis in post-operative patients: when and why. Haemostasis. 1999;29(5):247–254. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
