

Assessment of nerve involvement in the lumbar spine: agreement between magnetic resonance imaging, physical examination and pain drawing findings
- PMID: 20831785
- PMCID: PMC2944219
- DOI: 10.1186/1471-2474-11-202
Assessment of nerve involvement in the lumbar spine: agreement between magnetic resonance imaging, physical examination and pain drawing findings
Abstract
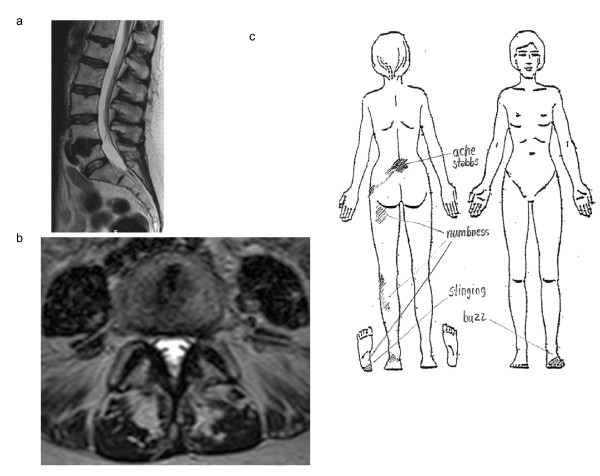
Background: Detection of nerve involvement originating in the spine is a primary concern in the assessment of spine symptoms. Magnetic resonance imaging (MRI) has become the diagnostic method of choice for this detection. However, the agreement between MRI and other diagnostic methods for detecting nerve involvement has not been fully evaluated. The aim of this diagnostic study was to evaluate the agreement between nerve involvement visible in MRI and findings of nerve involvement detected in a structured physical examination and a simplified pain drawing.
Methods: Sixty-one consecutive patients referred for MRI of the lumbar spine were - without knowledge of MRI findings - assessed for nerve involvement with a simplified pain drawing and a structured physical examination. Agreement between findings was calculated as overall agreement, the p value for McNemar's exact test, specificity, sensitivity, and positive and negative predictive values.
Results: MRI-visible nerve involvement was significantly less common than, and showed weak agreement with, physical examination and pain drawing findings of nerve involvement in corresponding body segments. In spine segment L4-5, where most findings of nerve involvement were detected, the mean sensitivity of MRI-visible nerve involvement to a positive neurological test in the physical examination ranged from 16-37%. The mean specificity of MRI-visible nerve involvement in the same segment ranged from 61-77%. Positive and negative predictive values of MRI-visible nerve involvement in segment L4-5 ranged from 22-78% and 28-56% respectively.
Conclusion: In patients with long-standing nerve root symptoms referred for lumbar MRI, MRI-visible nerve involvement significantly underestimates the presence of nerve involvement detected by a physical examination and a pain drawing. A structured physical examination and a simplified pain drawing may reveal that many patients with "MRI-invisible" lumbar symptoms need treatment aimed at nerve involvement. Factors other than present MRI-visible nerve involvement may be responsible for findings of nerve involvement in the physical examination and the pain drawing.
Figures

References
-
- Melton L. Taking a shot at neuropathic pain. The Lancet Neurology. 2003;2 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
