

Endocannabinoid involvement in endometriosis
- PMID: 20833475
- PMCID: PMC2972363
- DOI: 10.1016/j.pain.2010.08.037
Endocannabinoid involvement in endometriosis
Abstract
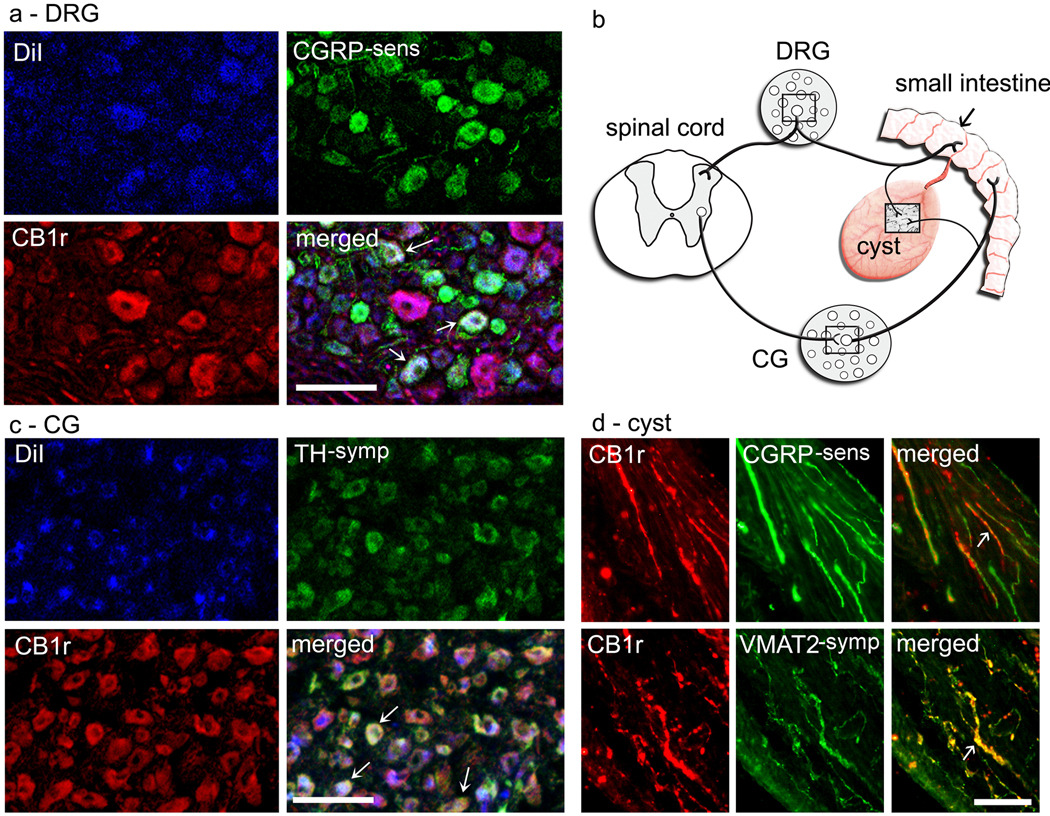
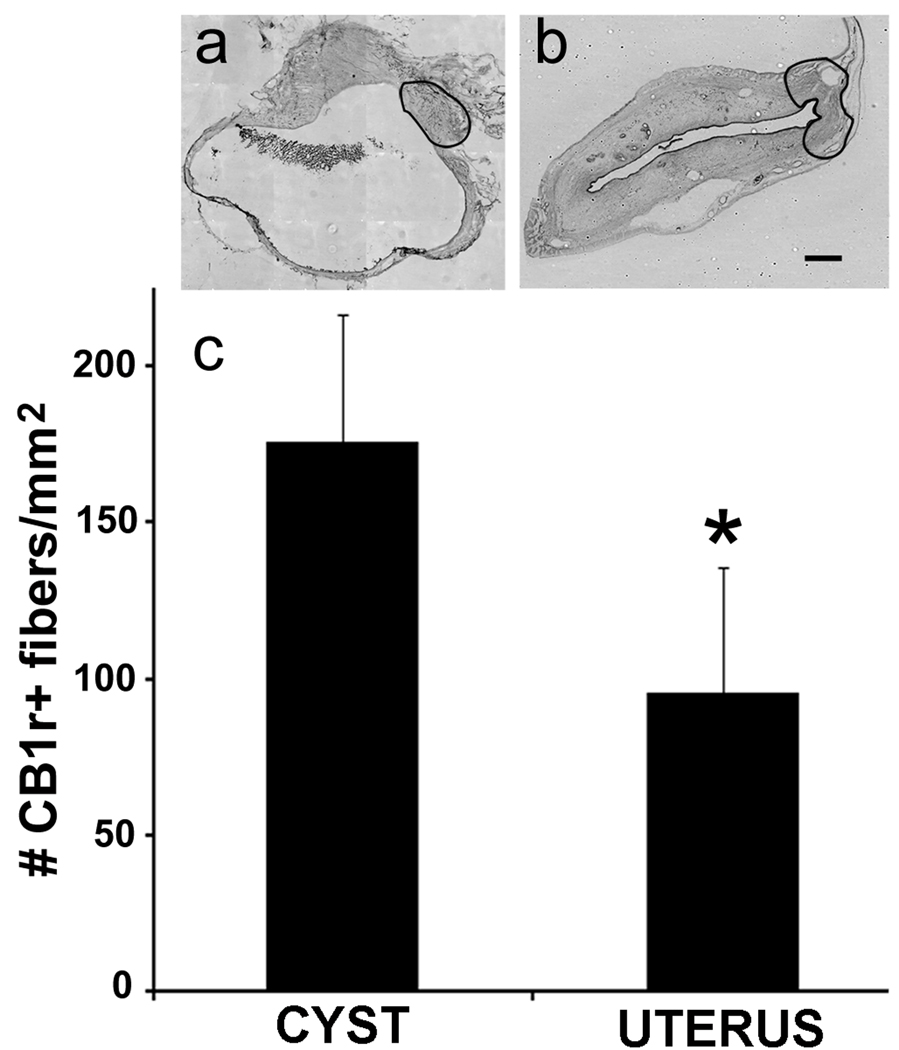
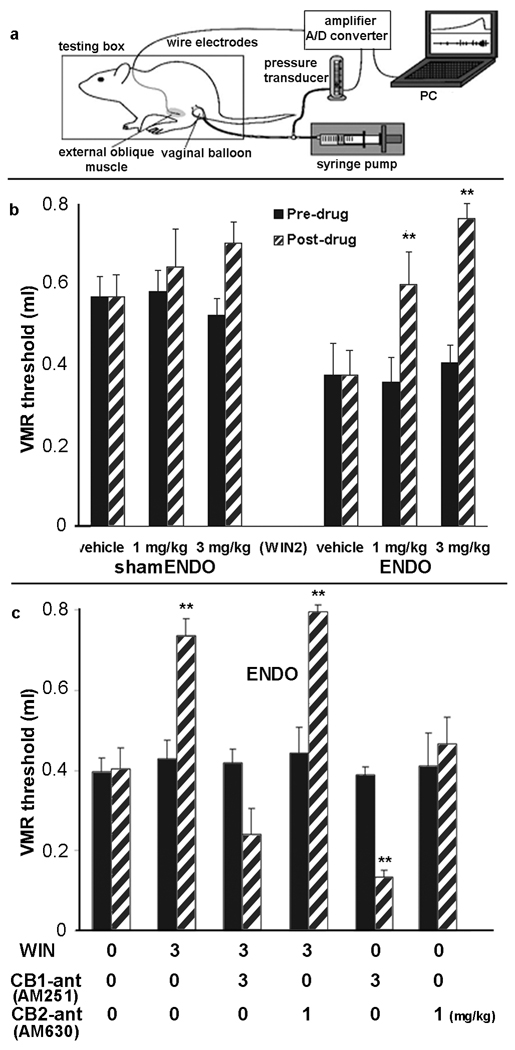
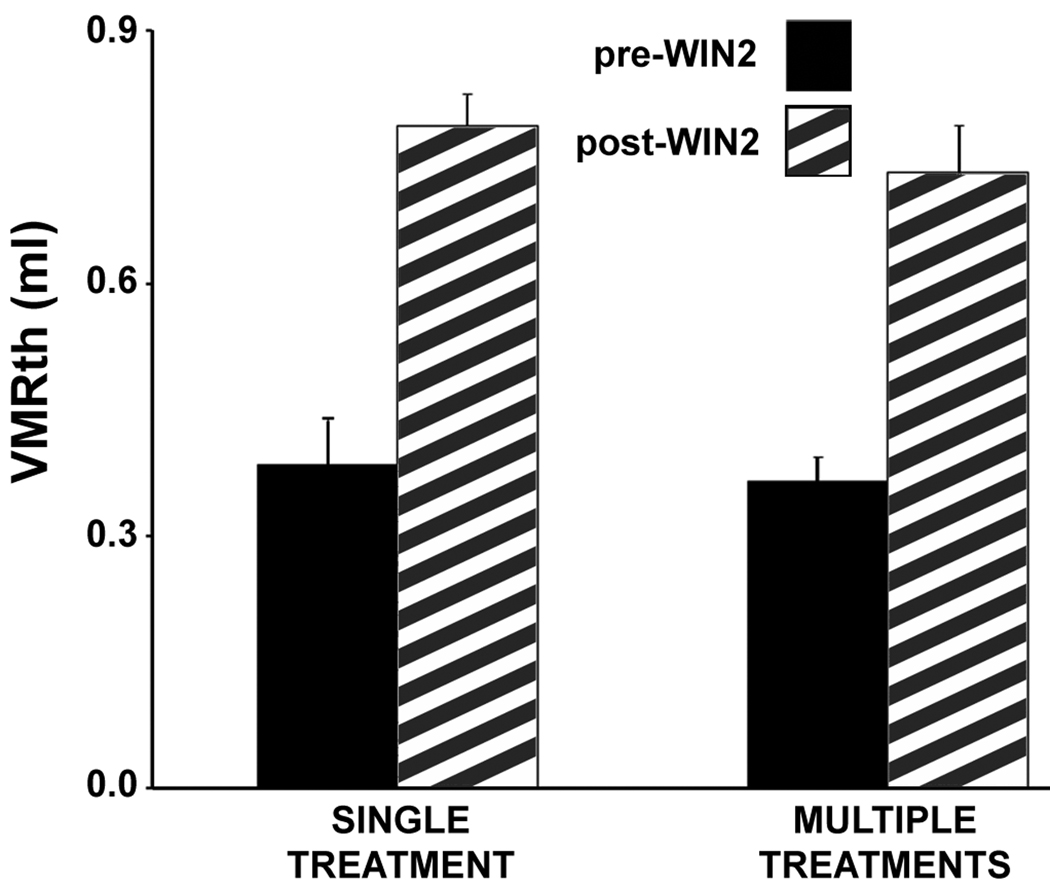
Endometriosis is a disease common in women that is defined by abnormal extrauteral growths of uterine endometrial tissue and associated with severe pain. Partly because how the abnormal growths become associated with pain is poorly understood, the pain is difficult to alleviate without resorting to hormones or surgery, which often produce intolerable side effects or fail to help. Recent studies in a rat model and women showed that sensory and sympathetic nerve fibers sprout branches to innervate the abnormal growths. This situation, together with knowledge that the endocannabinoid system is involved in uterine function and dysfunction and that exogenous cannabinoids were once used to alleviate endometriosis-associated pain, suggests that the endocannabinoid system is involved in both endometriosis and its associated pain. Herein, using a rat model, we found that CB1 cannabinoid receptors are expressed on both the somata and fibers of both the sensory and sympathetic neurons that innervate endometriosis's abnormal growths. We further found that CB1 receptor agonists decrease, whereas CB1 receptor antagonists increase, endometriosis-associated hyperalgesia. Together these findings suggest that the endocannabinoid system contributes to mechanisms underlying both the peripheral innervation of the abnormal growths and the pain associated with endometriosis, thereby providing a novel approach for the development of badly-needed new treatments.
Copyright © 2010 International Association for the Study of Pain. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Agarwal N, Pacher P, Tegeder I, Amaya F, Constantin CE, Brenner GJ, Rubino T, Michalski CW, Marsicano G, Monory K, Mackie K, Marian C, Batkai S, Parolaro D, Fischer MJ, Reeh P, Kunos G, Kress M, Lutz B, Woolf CJ, Kuner R. Cannabinoids mediate analgesia largely via peripheral type 1 cannabinoid receptors in nociceptors. Nat Neurosci. 2007;10:870–879. - PMC - PubMed
-
- Allen C, Hopewell S, Prentice A, Gregory D. Nonsteroidal anti-inflammatory drugs for pain in women with endometriosis. Cochrane Database Syst Rev. 2009;(2) CD004753. - PubMed
-
- Becker JB, Arnold AP, Berkley KJ, Blaustein JD, Eckel LA, Hampson E, Herman JP, Marts S, Sadee W, Steiner M, Taylor J, Young E. Strategies and methods for research on sex differences in brain and behavior. Endocrinology. 2005;146:1650–1673. - PubMed
-
- Berkley KJ, Rapkin AJ, Papka RE. The pains of endometriosis. Science. 2005;308:1587–1589. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
