

Cost-effectiveness of a day hospital falls prevention programme for screened community-dwelling older people at high risk of falls
- PMID: 20833862
- PMCID: PMC2956532
- DOI: 10.1093/ageing/afq108
Cost-effectiveness of a day hospital falls prevention programme for screened community-dwelling older people at high risk of falls
Abstract
Background: multifactorial falls prevention programmes for older people have been proved to reduce falls. However, evidence of their cost-effectiveness is mixed.
Design: economic evaluation alongside pragmatic randomised controlled trial.
Intervention: randomised trial of 364 people aged ≥70, living in the community, recruited via GP and identified as high risk of falling. Both arms received a falls prevention information leaflet. The intervention arm were also offered a (day hospital) multidisciplinary falls prevention programme, including physiotherapy, occupational therapy, nurse, medical review and referral to other specialists.
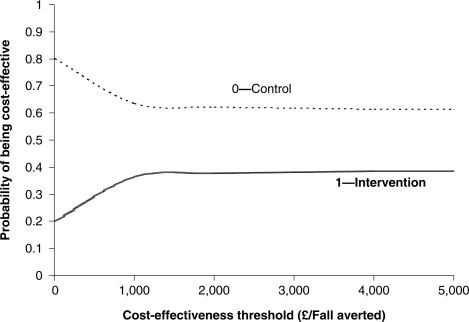
Measurements: self-reported falls, as collected in 12 monthly diaries. Levels of health resource use associated with the falls prevention programme, screening (both attributed to intervention arm only) and other health-care contacts were monitored. Mean NHS costs and falls per person per year were estimated for both arms, along with the incremental cost-effectiveness ratio (ICER) and cost effectiveness acceptability curve.
Results: in the base-case analysis, the mean falls programme cost was £349 per person. This, coupled with higher screening and other health-care costs, resulted in a mean incremental cost of £578 for the intervention arm. The mean falls rate was lower in the intervention arm (2.07 per person/year), compared with the control arm (2.24). The estimated ICER was £3,320 per fall averted.
Conclusions: the estimated ICER was £3,320 per fall averted. Future research should focus on adherence to the intervention and an assessment of impact on quality of life.
Comment in
-
Re: The impact of cognition on falls prevention programmes.Age Ageing. 2011 Sep;40(5):648; author reoly 648. doi: 10.1093/ageing/afr092. Age Ageing. 2011. PMID: 21835937 No abstract available.
References
-
- Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG, Rowe BH. Interventions for preventing falls in elderly people. Cochrane Database Syst Rev. 2001:CD000340. - PubMed
-
- Lamb SE. Scoping Exercise on Fallers’ Clinics, 2007.
-
- Masud T, Coupland C, Drummond A, et al. Multifactorial day hospital intervention to reduce falls in high risk older people in primary care: a multi-centre randomised controlled trial [ISRCTN46584556] Trials. 2006;7:5. doi:10.1186/1745-6215-7-5. - DOI - PMC - PubMed
-
- Conroy S. 2009. Preventing Falls in Older People. University of Nottingham.
-
- Anon. Avoiding Slips, Trips and Broken Hips. Department of Trade and Industry, ed. HMSO; 2001.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
