

Stimulant-responsive and stimulant-refractory aggressive behavior among children with ADHD
- PMID: 20837589
- PMCID: PMC2956067
- DOI: 10.1542/peds.2010-0086
Stimulant-responsive and stimulant-refractory aggressive behavior among children with ADHD
Abstract
Objectives: The objective of this study was to examine factors that are associated with aggression that is responsive versus refractory to individualized optimization of stimulant monotherapy among children with attention-deficit/hyperactivity disorder (ADHD).
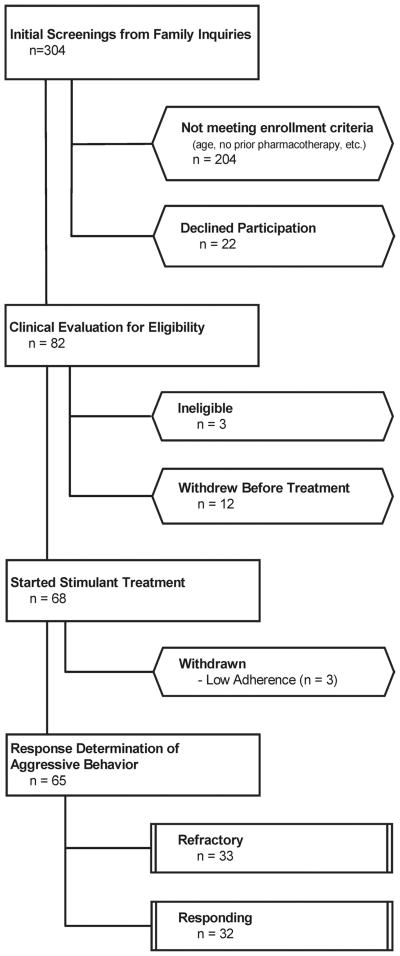
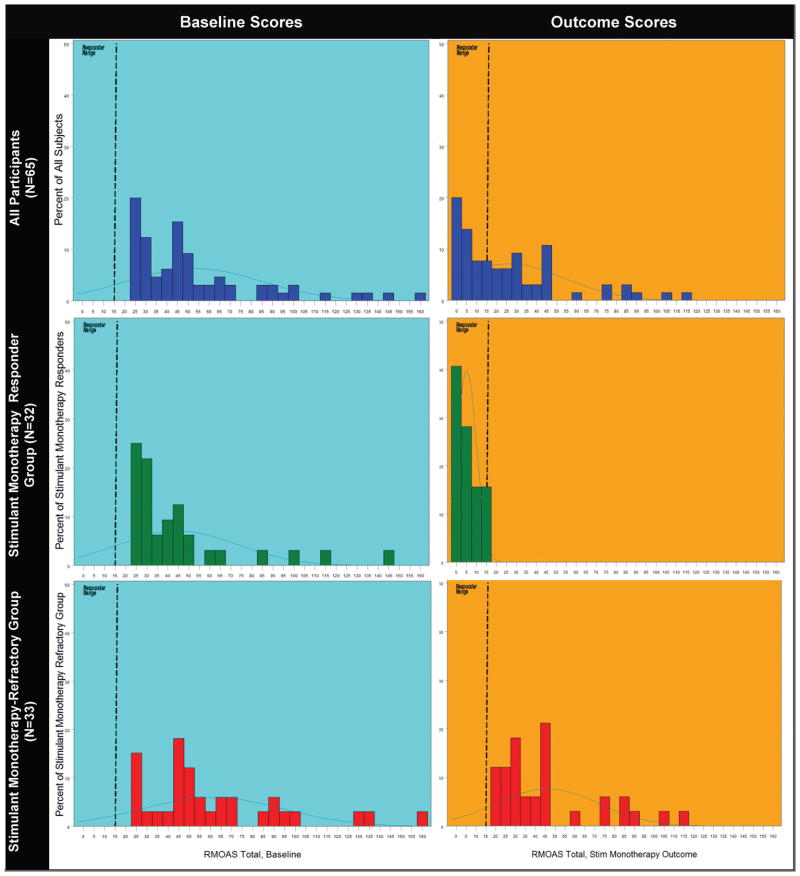
Methods: Children who were aged 6 to 13 years and had ADHD, either oppositional defiant disorder or conduct disorder, significant aggressive behavior, and a history of insufficient response to stimulants completed an open stimulant monotherapy optimization protocol. Stimulant titration with weekly assessments of behavior and tolerability identified an optimal regimen for each child. Families also received behavioral therapy. Parents completed the Retrospective-Modified Overt Aggression Scale (R-MOAS) at each visit. Children were classified as having stimulant-refractory aggression on the basis of R-MOAS ratings and clinician judgment. Differences that pertained to treatment, demographic, and psychopathology between groups with stimulant monotherapy-responsive and -refractory aggression were evaluated.
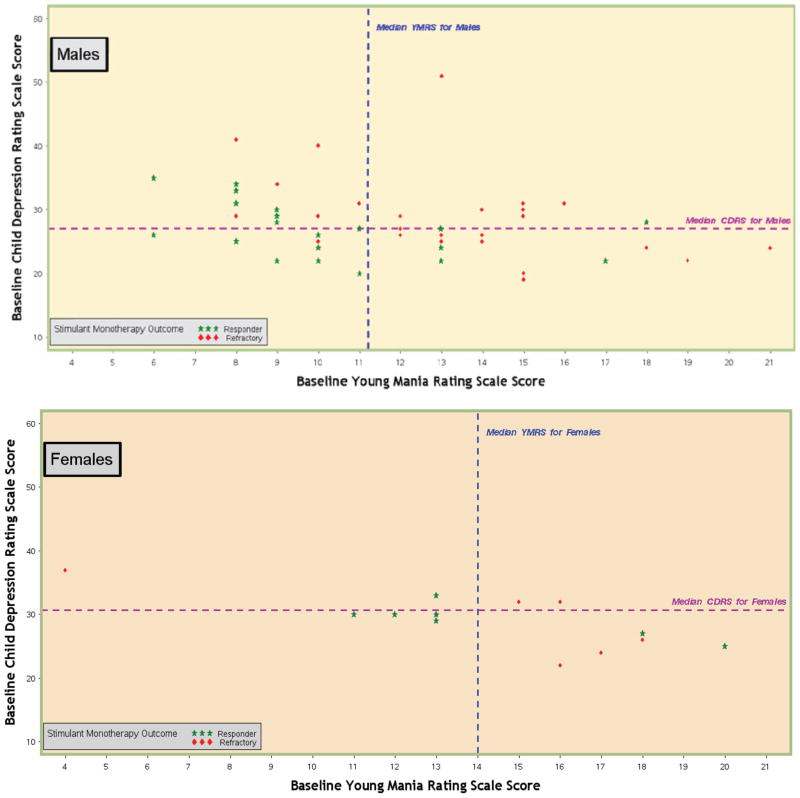
Results: Aggression among 32 (49.3%) of 65 children was reduced sufficiently after stimulant dosage adjustment and behavioral therapy to preclude adjunctive medication. Those who responded to stimulant monotherapy were more likely to benefit from the protocol's methylphenidate preparation (once-daily, triphasic release), showed a trend for lower average dosages, and received fewer behavioral therapy sessions than did children with stimulant-refractory aggression. Boys, especially those with higher ratings of baseline aggression and of depressive and manic symptoms, more often exhibited stimulant-refractory aggression.
Conclusions: Among children whose aggressive behavior develops in the context of ADHD and of oppositional defiant disorder or conduct disorder, and who had insufficient response to previous stimulant treatment in routine clinical care, systematic, well-monitored titration of stimulant monotherapy often culminates in reduced aggression that averts the need for additional agents.
Figures
References
-
- Brown RT, Amler RW, Freeman WS, et al. Treatment of attention-deficit/hyperactivity disorder: overview of the evidence. Pediatrics. 2005. Available at: www.pediatrics.org/cgi/content/full/115/6/e749. - PubMed
-
- Greenhill LL, Halperin JM, Abikoff H. Stimulant medications. J Am Acad Child Adolesc Psychiatry. 1999;38(5):503–512. - PubMed
-
- Klein RG, Abikoff H, Klass E, Ganeles D, Seese LM, Pollack S. Clinical efficacy of methylphenidate in conduct disorder with and without attention deficit hyperactivity disorder. Arch Gen Psychiatry. 1997;54(12):1073–1080. - PubMed
-
- Connor D, Glatt S, Lopez I, Jackson D, Melloni R. Psychopharmacology and aggression: I—a meta-analysis of stimulant effects on overt/covert aggression: related behaviors in ADHD. J Am Acad Child Adolesc Psychiatry. 2002;41(3):253–261. - PubMed
-
- Olfson M, Blanco C, Liu L, Moreno C, Laje G. National trends in the outpatient treatment of children and adolescents with antipsychotic drugs. Arch Gen Psychiatry. 2006;63(6):679–685. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
