

Triiodothyronine Supplementation in Infants and Children Undergoing Cardiopulmonary Bypass (TRICC): a multicenter placebo-controlled randomized trial: age analysis
- PMID: 20837917
- PMCID: PMC3090076
- DOI: 10.1161/CIRCULATIONAHA.109.926394
Triiodothyronine Supplementation in Infants and Children Undergoing Cardiopulmonary Bypass (TRICC): a multicenter placebo-controlled randomized trial: age analysis
Abstract
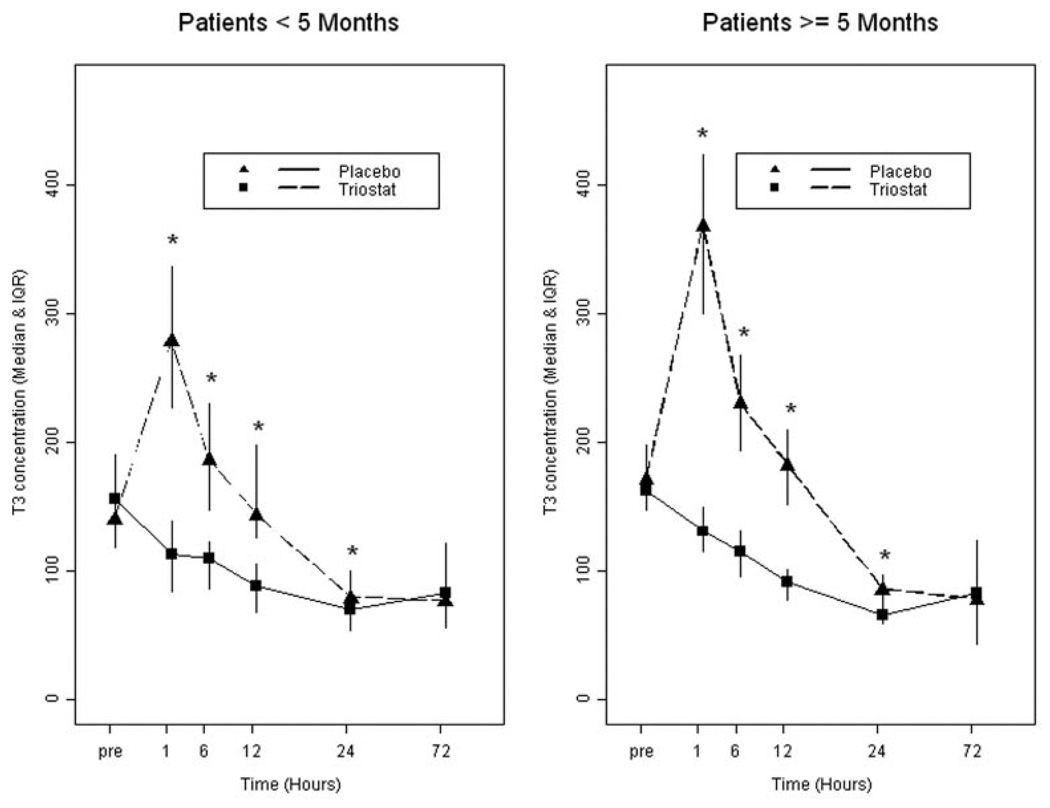
Background: Triiodothyronine levels decrease in infants and children after cardiopulmonary bypass. We tested the primary hypothesis that triiodothyronine (T3) repletion is safe in this population and produces improvements in postoperative clinical outcome.
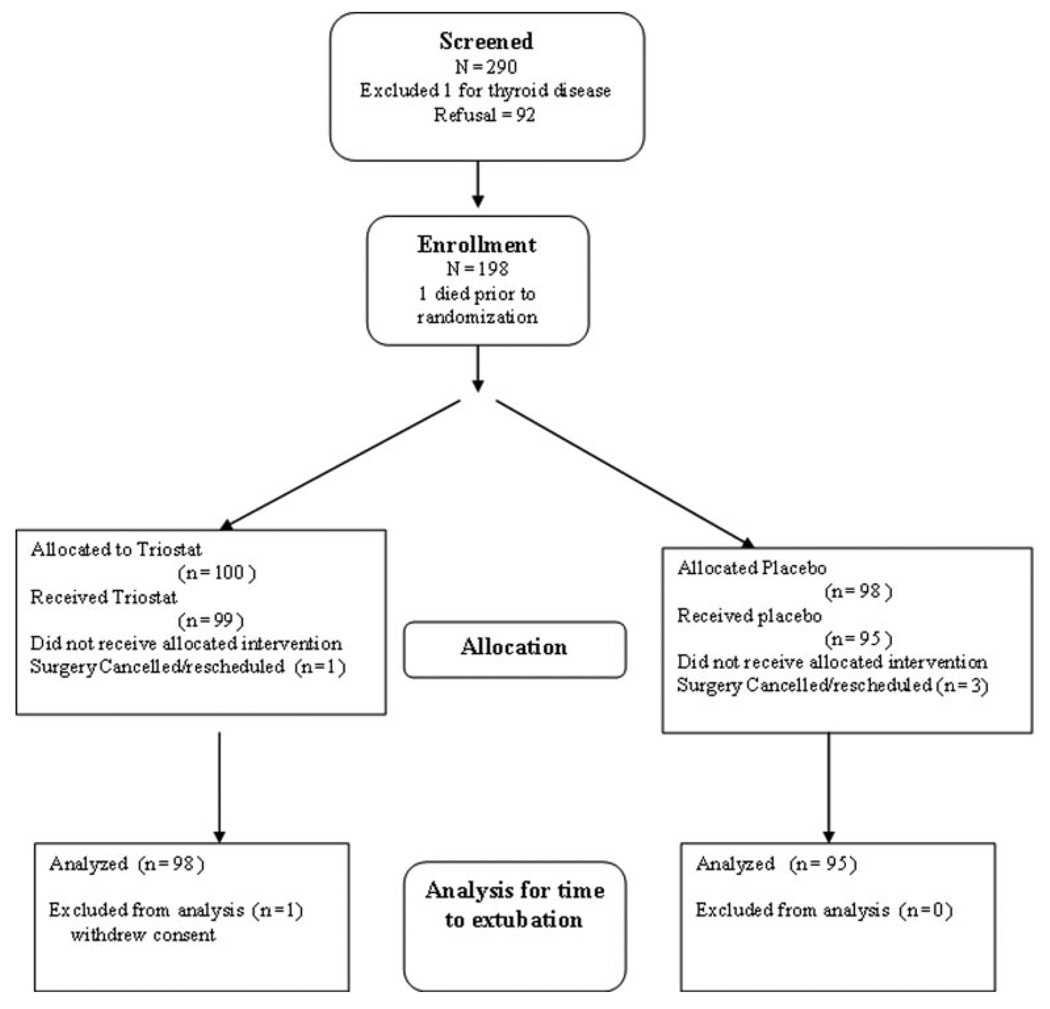
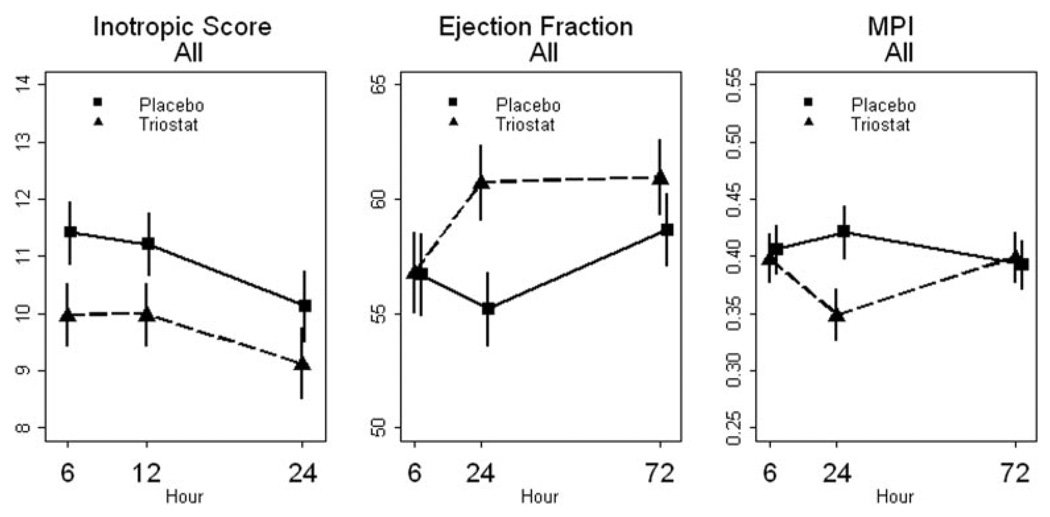
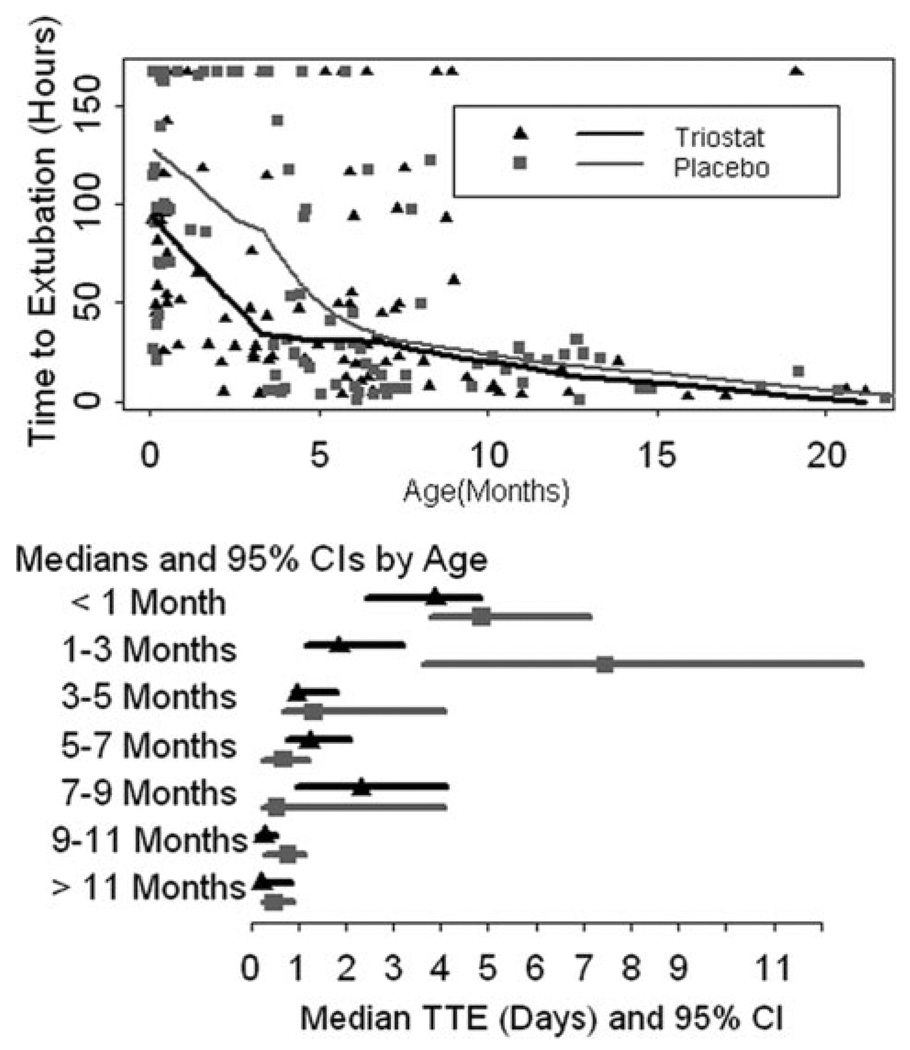
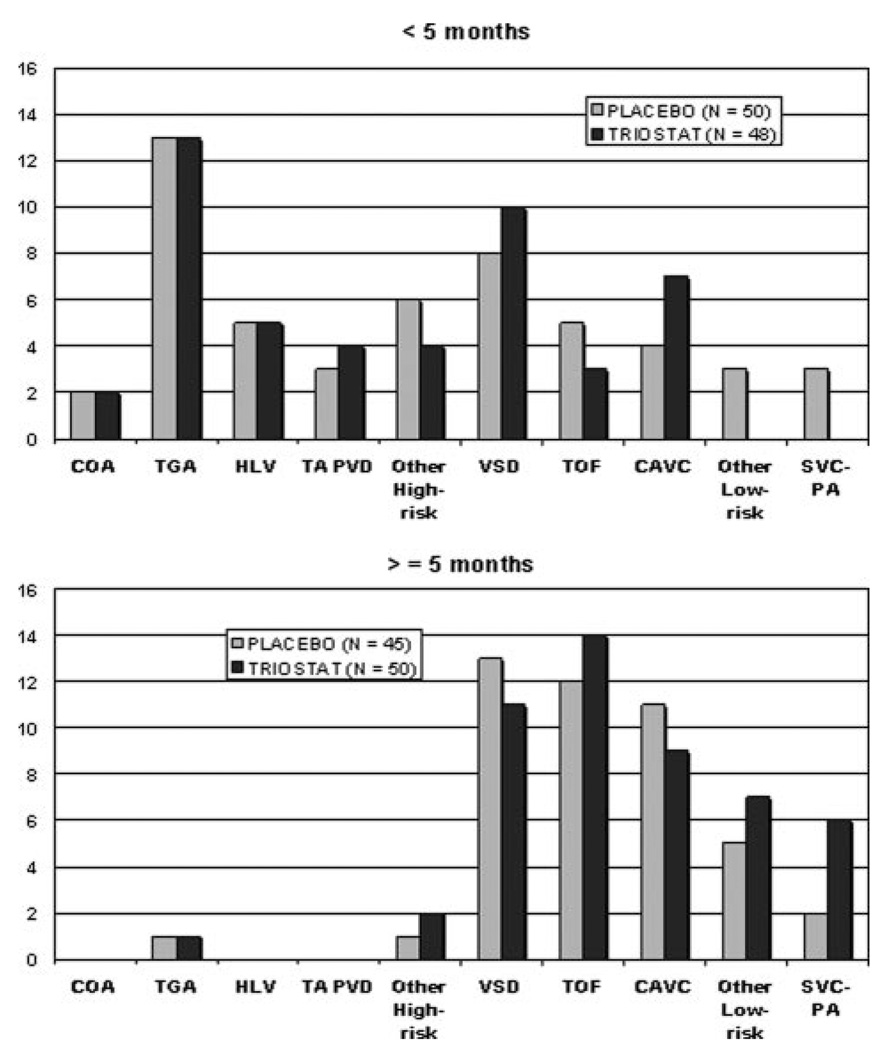
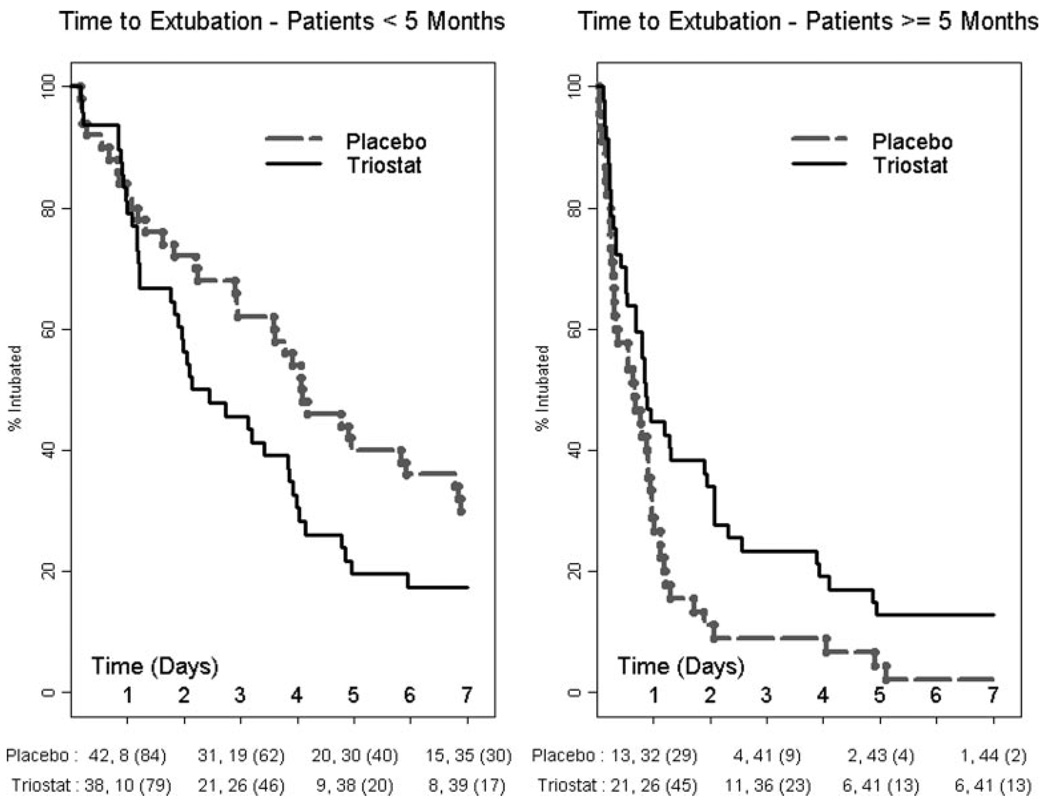
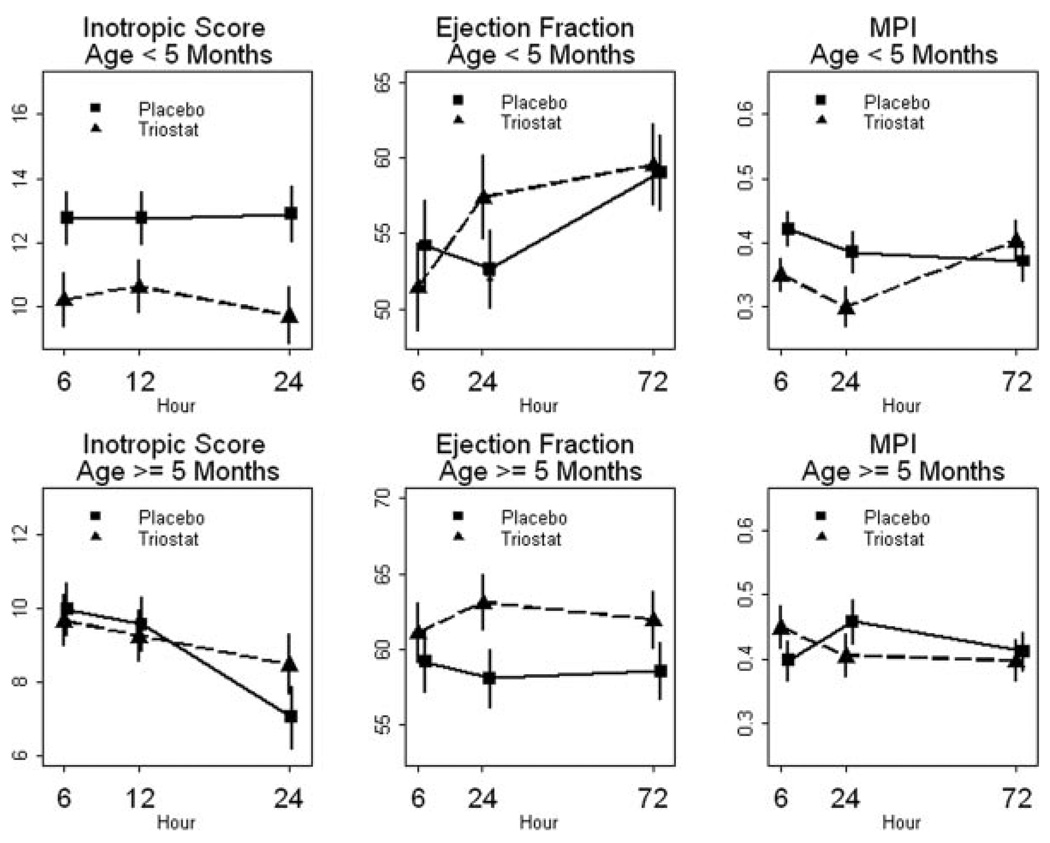
Methods and results: The TRICC study was a prospective, multicenter, double-blind, randomized, placebo-controlled trial in children younger than 2 years old undergoing heart surgery with cardiopulmonary bypass. Enrollment was stratified by surgical diagnosis. Time to extubation (TTE) was the primary outcome. Patients received intravenous T3 as Triostat (n=98) or placebo (n=95), and data were analyzed using Cox proportional hazards. Overall, TTE was similar between groups. There were no differences in adverse event rates, including arrhythmia. Prespecified analyses showed a significant interaction between age and treatment (P=0.0012). For patients younger than 5 months, the hazard ratio (chance of extubation) for Triostat was 1.72. (P=0.0216). Placebo median TTE was 98 hours with 95% confidence interval (CI) of 71 to 142 compared to Triostat TTE at 55 hours with CI of 44 to 92. TTE shortening corresponded to a reduction in inotropic agent use and improvement in cardiac function. For children 5 months of age, or older, Triostat produced a significant delay in median TTE: 16 hours (CI, 7-22) for placebo and 20 hours (CI, 16-45) for Triostat and (hazard ratio, 0.60; P=0.0220).
Conclusions: T3 supplementation is safe. Analyses using age stratification indicate that T3 supplementation provides clinical advantages in patients younger than 5 months and no benefit for those older than 5 months. Clinical Trial Registration-URL: http://www.clinicaltrials.gov. Unique identifier: NCT00027417.
Figures
References
-
- Bettendorf M, Schmidt KG, Tiefenbacher U, Grulich-Henn J, Heinrich UE, Schonberg DK. Transient secondary hypothyroidism in children after cardiac surgery. Pediatr Res. 1997;41:375–379. - PubMed
-
- Klemperer JD, Klein I, Gomez M, Helm RE, Ojamaa K, Thomas SJ, Isom OW, Krieger K. Thyroid hormone treatment after coronary-artery bypass surgery. N Engl J Med. 1995;333:1522–1527. - PubMed
-
- Klemperer JD, Klein IL, Ojamaa K, Helm RE, Gomez M, Isom OW, Krieger KH. Triiodothyronine therapy lowers the incidence of atrial fibrillation after cardiac operations. Ann Thorac Surg. 1996;61:1323–1327. discussion 1328–1329. - PubMed
-
- Mullis-Jansson SL, Argenziano M, Corwin S, Homma S, Weinberg AD, Williams M, Rose EA, Smith CR. A randomized double-blind study of the effect of triiodothyronine on cardiac function and morbidity after coronary bypass surgery. J Thorac Cardiovasc Surg. 1999;117:1128–1134. - PubMed
-
- Plumpton K, Haas NA. Identifying infants at risk of marked thyroid suppression post-cardiopulmonary bypass. Intensive Care Med. 2005;31:581–587. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
