

Place of death: correlations with quality of life of patients with cancer and predictors of bereaved caregivers' mental health
- PMID: 20837950
- PMCID: PMC2988637
- DOI: 10.1200/JCO.2009.26.3863
Place of death: correlations with quality of life of patients with cancer and predictors of bereaved caregivers' mental health
Abstract
Purpose: To determine whether the place of death for patients with cancer is associated with patients' quality of life (QoL) at the end of life (EOL) and psychiatric disorders in bereaved caregivers.
Patients and methods: Prospective, longitudinal, multisite study of patients with advanced cancer and their caregivers (n = 342 dyads). Patients were followed from enrollment to death, a median of 4.5 months later. Patients' QoL at the EOL was assessed by caregiver report within 2 weeks of death. Bereaved caregivers' mental health was assessed at baseline and 6 months after loss with the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, and the Prolonged Grief Disorder interview.
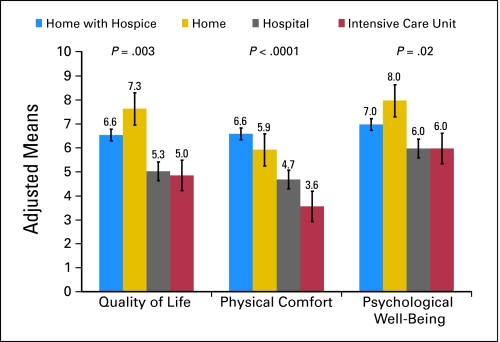
Results: In adjusted analyses, patients with cancer who died in an intensive care unit (ICU) or hospital experienced more physical and emotional distress and worse QoL at the EOL (all P ≤ .03), compared with patients who died at home with hospice. ICU deaths were associated with a heightened risk for posttraumatic stress disorder, compared with home hospice deaths (21.1% [four of 19] v 4.4% [six of 137]; adjusted odds ratio [AOR], 5.00; 95% CI, 1.26 to 19.91; P = .02), after adjustment for caregivers' preexisting psychiatric illnesses. Similarly, hospital deaths were associated with a heightened risk for prolonged grief disorder (21.6% [eight of 37] v 5.2% [four of 77], AOR, 8.83; 95% CI, 1.51 to 51.77; P = .02), compared with home hospice deaths.
Conclusion: Patients with cancer who die in a hospital or ICU have worse QoL compared with those who die at home, and their bereaved caregivers are at increased risk for developing psychiatric illness. Interventions aimed at decreasing terminal hospitalizations or increasing hospice utilization may enhance patients' QoL at the EOL and minimize bereavement-related distress.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
References
-
- Earle CC, Neville BA, Landrum MB, et al. Trends in the aggressiveness of cancer care near the end of life. J Clin Oncol. 2004;22:315–321. - PubMed
-
- Emanuel EJ, Young-Xu Y, Levinsky NG, et al. Chemotherapy use among Medicare beneficiaries at the end of life. Ann Intern Med. 2003;138:639–643. - PubMed
-
- Temel JS, McCanon J, Greer JA, et al. Aggressiveness of care in a prospective cohort of patients with advanced NSCLC. Cancer. 2008;113:826–833. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
