

Cost-effectiveness analysis of combination therapies for visceral leishmaniasis in the Indian subcontinent
- PMID: 20838649
- PMCID: PMC2935395
- DOI: 10.1371/journal.pntd.0000818
Cost-effectiveness analysis of combination therapies for visceral leishmaniasis in the Indian subcontinent
Abstract
Background: Visceral leishmaniasis is a systemic parasitic disease that is fatal unless treated. We assessed the cost and cost-effectiveness of alternative strategies for the treatment of visceral leishmaniasis in the Indian subcontinent. In particular we examined whether combination therapies are a cost-effective alternative compared to monotherapies.
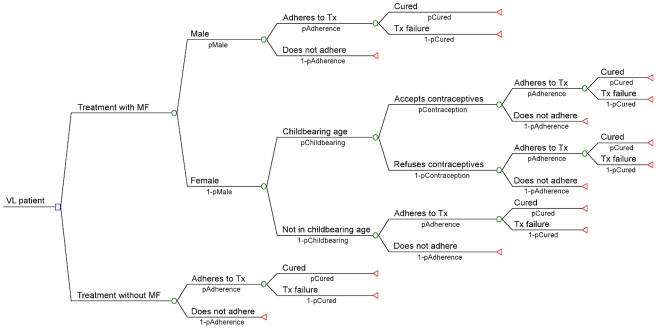
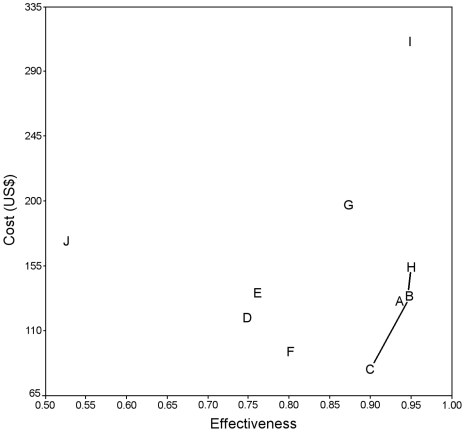
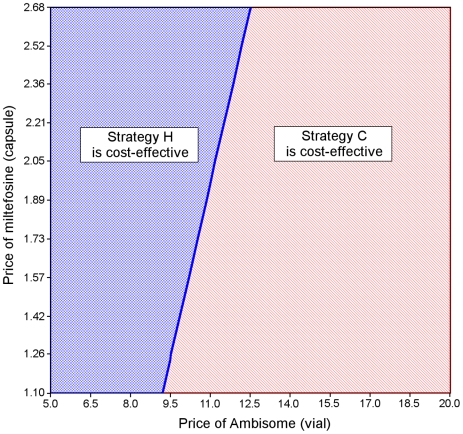
Methods and findings: We assessed the cost-effectiveness of all possible mono- and combination therapies for the treatment of visceral leishmaniasis in the Indian subcontinent (India, Nepal and Bangladesh) from a societal perspective using a decision analytical model based on a decision tree. Primary data collected in each country was combined with data from the literature and an expert poll (Delphi method). The cost per patient treated and average and incremental cost-effectiveness ratios expressed as cost per death averted were calculated. Extensive sensitivity analysis was done to evaluate the robustness of our estimations and conclusions. With a cost of US$92 per death averted, the combination miltefosine-paromomycin was the most cost-effective treatment strategy. The next best alternative was a combination of liposomal amphotericin B with paromomycin with an incremental cost-effectiveness of $652 per death averted. All other strategies were dominated with the exception of a single dose of 10mg per kg of liposomal amphotericin B. While strategies based on liposomal amphotericin B (AmBisome) were found to be the most effective, its current drug cost of US$20 per vial resulted in a higher average cost-effectiveness. Sensitivity analysis showed the conclusion to be robust to variations in the input parameters over their plausible range.
Conclusions: Combination treatments are a cost-effective alternative to current monotherapy for VL. Given their expected impact on the emergence of drug resistance, a switch to combination therapy should be considered once final results from clinical trials are available.
Conflict of interest statement
All authors declare that there are no conflicts of interest. The opinions expressed in this paper are those of the authors and may not reflect those of their employing organizations. PO is a staff member of the WHO; the authors alone are responsible for the views expressed in this publication and they do not necessarily represent the decisions, policy or views of the WHO.
Figures
References
-
- Sundar S, More DK, Singh MK, Singh VP, Sharma S, et al. Failure of pentavalent antimony in visceral leishmaniasis in India: report from the center of the Indian epidemic. Clin Infect Dis. 2000;31:1104–1107. - PubMed
-
- Rijal S, Chappuis F, Singh R, Bovier PA, Acharya P, et al. Treatment of visceral leishmaniasis in south-eastern Nepal: decreasing efficacy of sodium stibogluconate and need for a policy to limit further decline. Trans R Soc Trop Med Hyg. 2003;97:350–354. - PubMed
-
- Sundar S, Mondal D, Rijal S, Bhattacharya S, Ghalib H, et al. Implementation research to support the initiative on the elimination of kala azar from Bangladesh, India and Nepal–the challenges for diagnosis and treatment. Trop Med Int Health. 2008;13:2–5. - PubMed
-
- World Health Organization. Regional Strategic Framework for Elimination of Kala-azar from the South-East Asia Region (2005–2015) New Delhi: WHO Regional Office for South-East Asia; 2005.
-
- Sundar S, Jha TK, Thakur CP, Sinha PK, Bhattacharya SK. Injectable paromomycin for Visceral leishmaniasis in India. N Engl J Med. 2007;356:2571–2581. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
