

A multi-level analysis of non-significant counseling effects in a randomized smoking cessation trial
- PMID: 20840173
- PMCID: PMC2975757
- DOI: 10.1111/j.1360-0443.2010.03089.x
A multi-level analysis of non-significant counseling effects in a randomized smoking cessation trial
Abstract
Aims: To determine, in the context of a trial in which counseling did not improve smoking cessation outcomes, whether this was due to a failure of the conceptual theory identifying treatment targets or the action theory specifying interventions.
Design: Data from a randomized clinical trial of smoking cessation counseling and bupropion SR were submitted to multi-level modeling to test whether counseling influenced real-time reports of cognitions, emotions and behaviors, and whether these targets predicted abstinence.
Setting: Center for Tobacco Research and Intervention, Madison, WI.
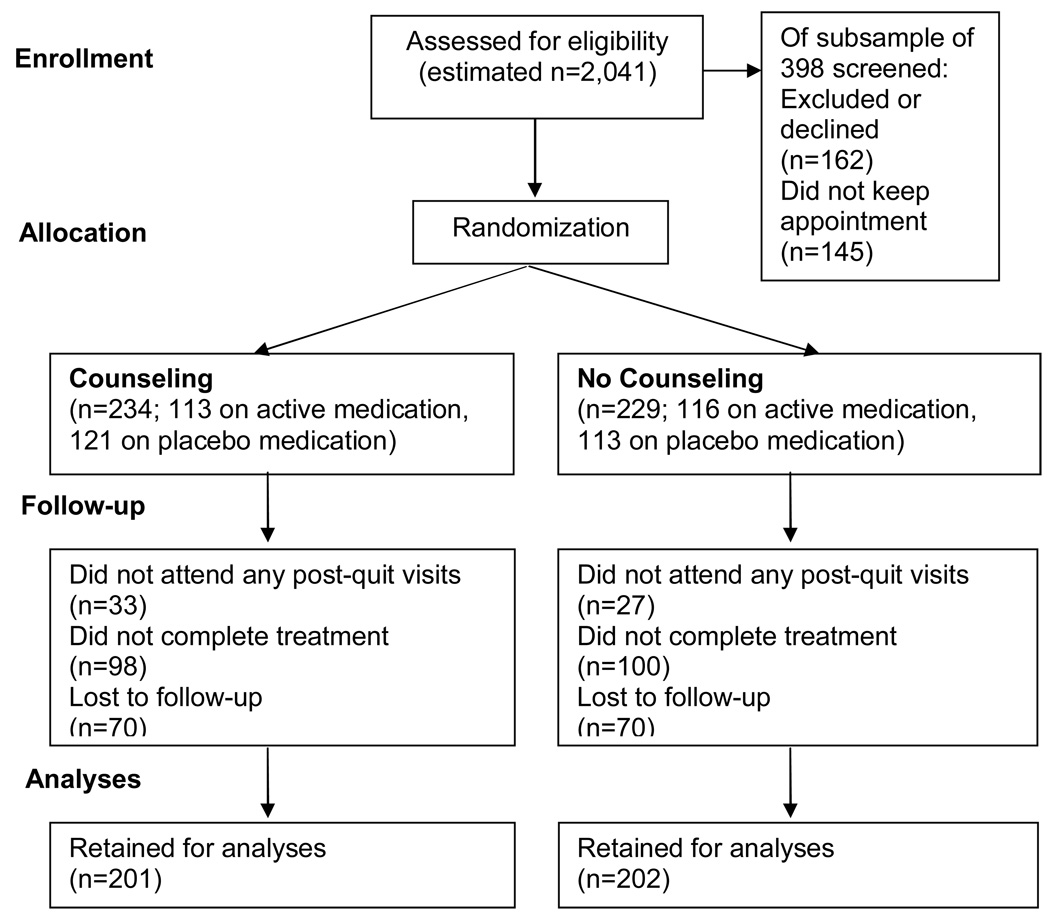
Participants: A total of 403 adult, daily smokers without contraindications to bupropion SR use. Participants were assigned randomly to receive individual counseling or no counseling and a 9-week course of bupropion SR or placebo pill. Cessation counseling was delivered in eight 10-minute sessions focused on bolstering social support, motivation, problem-solving and coping skills.
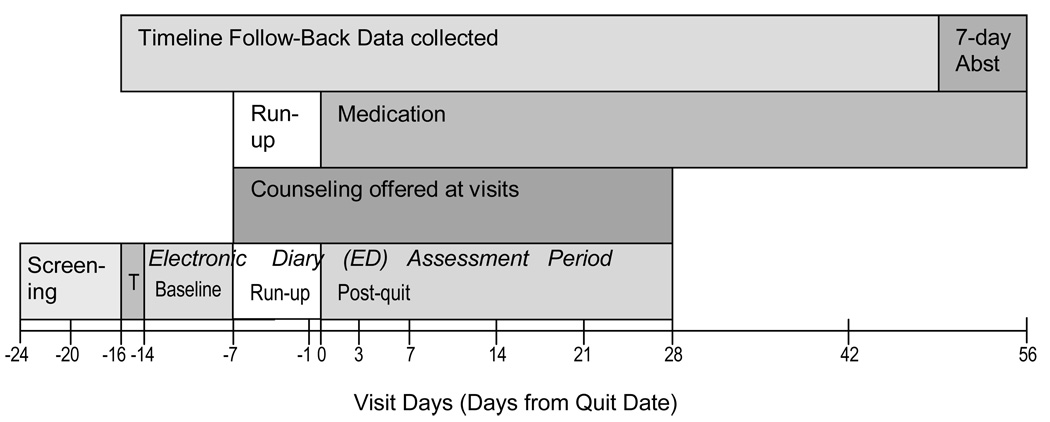
Measurements: Pre- and post-quit ecological momentary assessments of smoking behavior, smoking triggers, active prevention and coping strategies, motivation to quit, difficulty quitting and reactions to initial lapses.
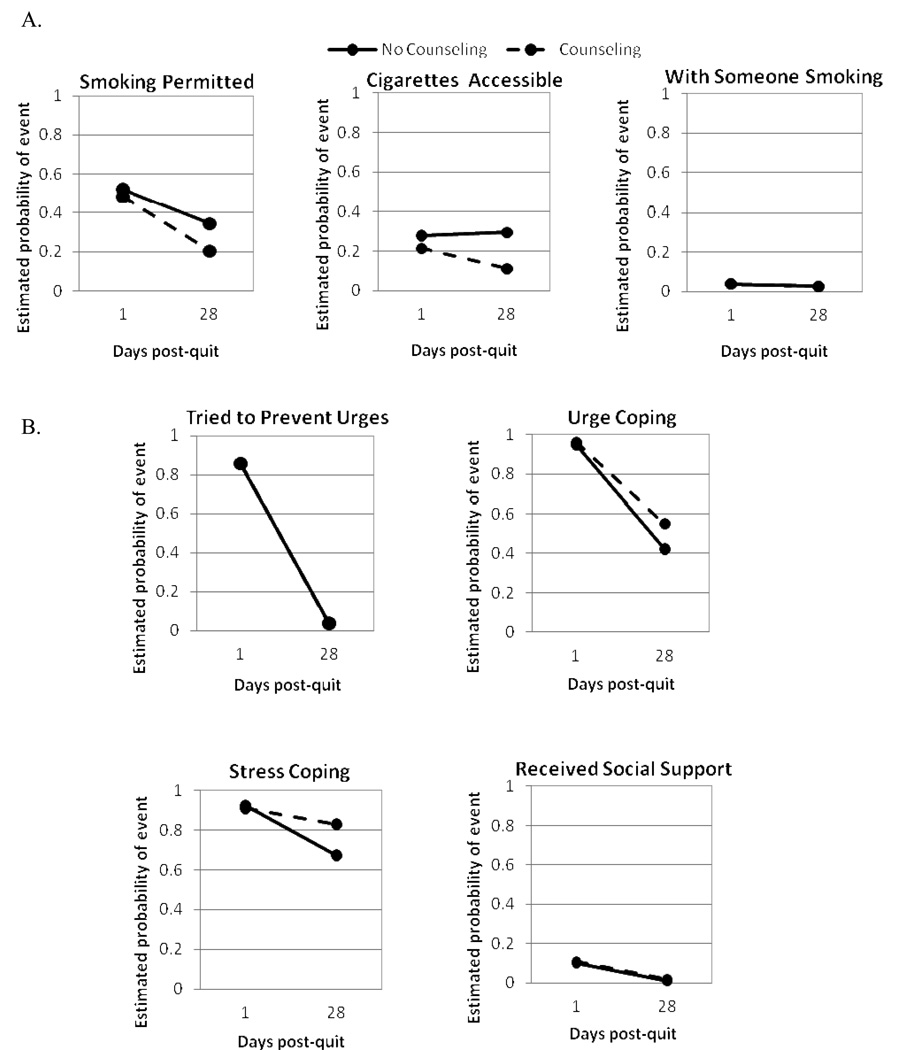
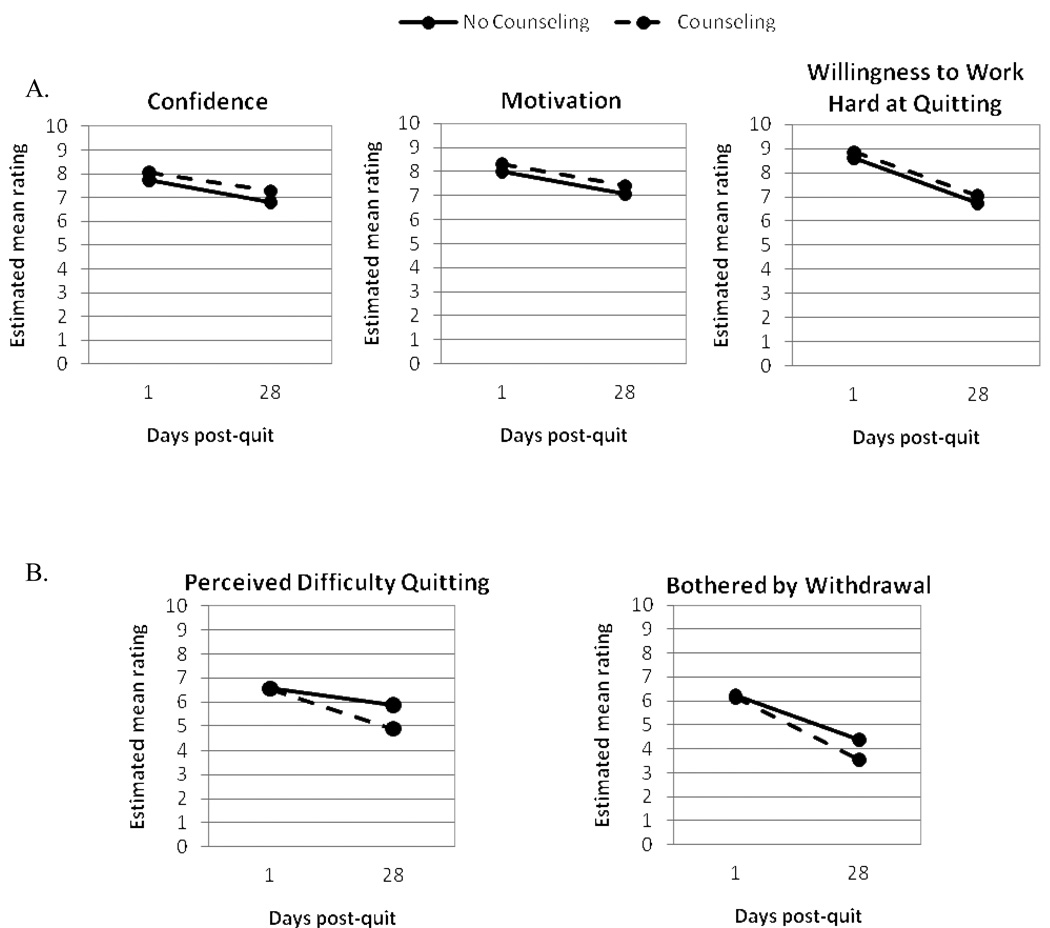
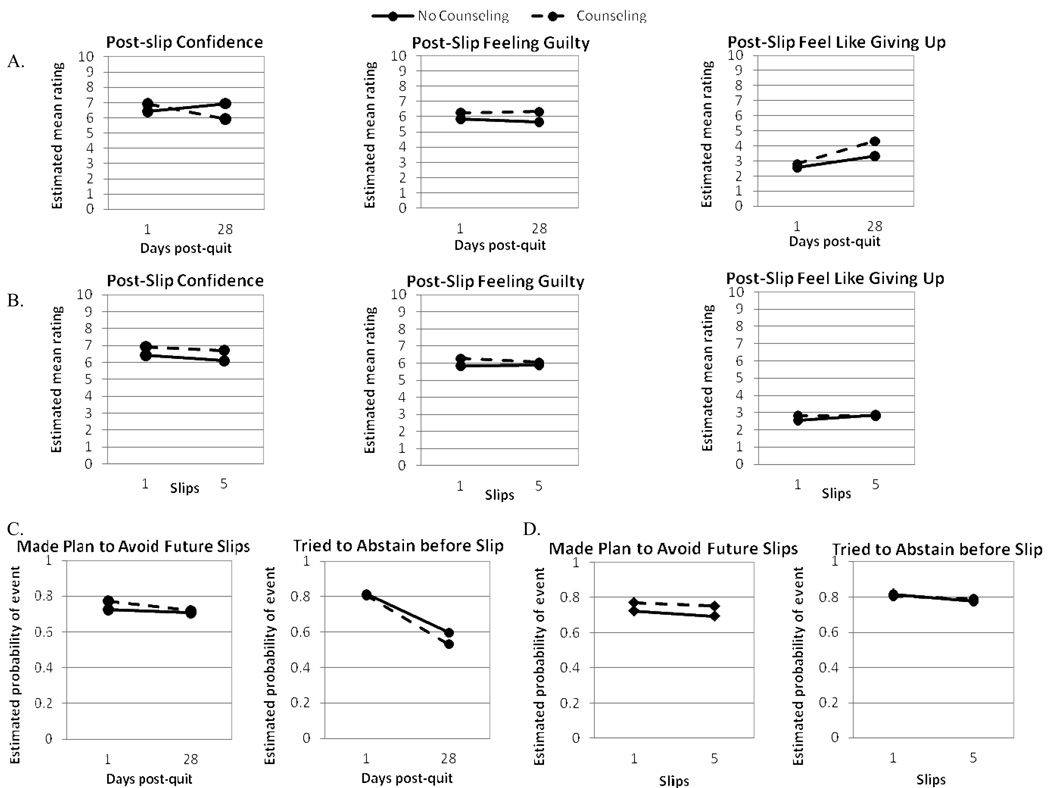
Findings: Counseling prompted avoidance of access to cigarettes, improved quitting self-efficacy, reduced perceived difficulty of quitting over time and protected against guilt and demoralization following lapses. Results also supported the importance of limiting cigarette access, receiving social support, strong motivation and confidence and easing withdrawal distress during cessation efforts. Quitting self-efficacy and perceived difficulty quitting may partially mediate counseling effects on abstinence.
Conclusions: Smoking cessation counseling may work by supporting confidence about quitting and reducing perceived difficulty quitting. Counseling did not affect other targets that protect against relapse.
© 2010 The Authors, Addiction © 2010 Society for the Study of Addiction.
Figures
References
-
- Fiore MC, Jaén CR, Baker TB, et al. Treating Tobacco Use and Dependence: 2008 Update. Clinical Practice Guideline. Rockville, MD: U.S. Department of Health and Human Services, Public Health Service; May, 2008.
-
- Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. The Cochrane Database of Systematic Reviews. 2005;(Issue 2) - PubMed
-
- Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database of Systematic Reviews. 2005;(Issue 1) - PubMed
-
- Stead LF, Perera R, Lancaster T. Telephone counseling for smoking cessation. Cochrane Database of Systematic Reviews. 2006;(Issue 1) - PubMed
-
- MacLeod ZR, Charles MA, Arnaldi VC, Adams IM. Telephone counseling as an adjunct to nicotine patches in smoking cessation: a randomized controlled trial. Med J Australia. 2003;179:349–352. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
