

Buccal mucosa carcinoma: surgical margin less than 3 mm, not 5 mm, predicts locoregional recurrence
- PMID: 20840791
- PMCID: PMC2946296
- DOI: 10.1186/1748-717X-5-79
Buccal mucosa carcinoma: surgical margin less than 3 mm, not 5 mm, predicts locoregional recurrence
Abstract
Background: Most treatment failure of buccal mucosal cancer post surgery is locoregional recurrence. We tried to figure out how close the surgical margin being unsafe and needed further adjuvant treatment.
Methods: Between August 2000 and June 2008, a total of 110 patients with buccal mucosa carcinoma (25 with stage I, 31 with stage II, 11 with stage III, and 43 with Stage IV classified according to the American Joint Committee on Cancer 6th edition) were treated with surgery alone (n = 32), surgery plus postoperative radiotherapy (n = 38) or surgery plus adjuvant concurrent chemoradiotherapy (n = 40).
Main outcome measures: The primary endpoint was locoregional disease control.
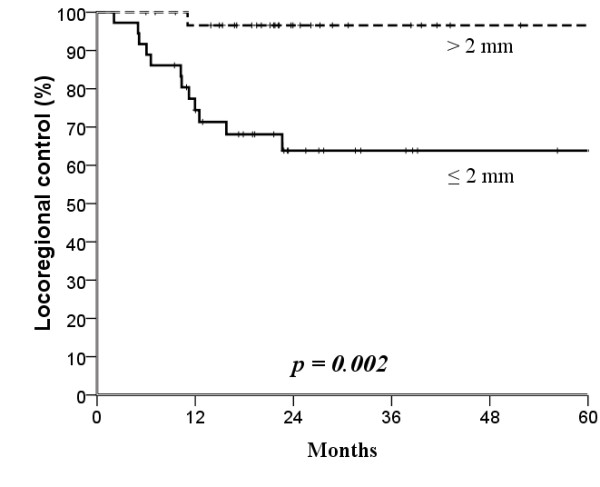
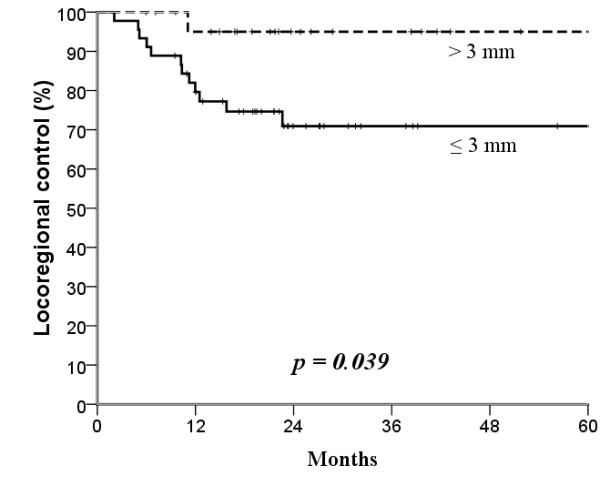
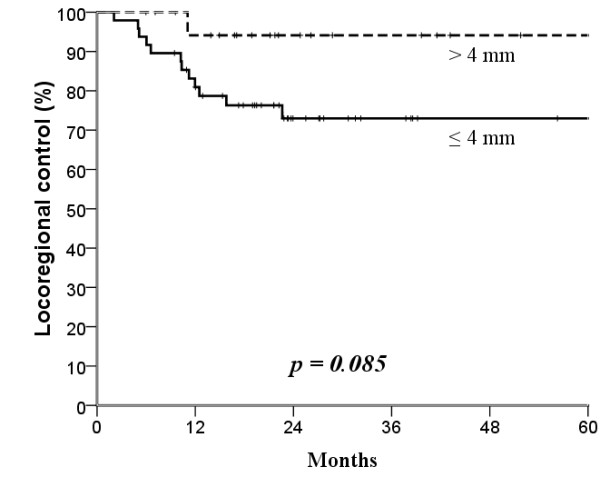
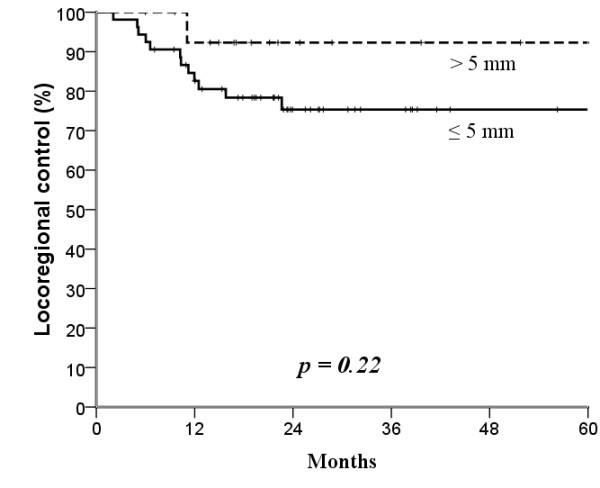
Results: The median follow-up time at analysis was 25 months (range, 4-104 months). The 3-year locoregional control rates were significantly different when a 3-mm surgical margin (≤3 versus >3 mm, 71% versus 95%, p = 0.04) but not a 5-mm margin (75% versus 92%, p = 0.22) was used as the cut-off level. We also found a quantitative correlation between surgical margin and locoregional failure (hazard ratio, 2.16; 95% confidence interval, 1.14 - 4.11; p = 0.019). Multivariate analysis identified pN classification and surgical margin as independent factors affecting disease-free survival and locoregional control.
Conclusions: Narrow surgical margin ≤3 mm, but not 5 mm, is associated with high risk for locoregional recurrence of buccal mucosa carcinoma. More aggressive treatment after surgery is suggested.
Figures
References
-
- Franceschi S, Talamini R, Barra S, Baron AE, Negri E, Bidoli E, Serraino D, La Vecchia C. Smoking and drinking in relation to cancers of the oral cavity, pharynx, larynx, and esophagus in northern Italy. Cancer Res. 1990;50:6502–6507. - PubMed
-
- Lin YS, Jen YM, Wang BB, Lee JC, Kang BH. Epidemiology of oral cavity cancer in taiwan with emphasis on the role of betel nut chewing. ORL J Otorhinolaryngol Relat Spec. 2005;67:230–236. - PubMed
-
- Lapeyre M, Peiffert D, Malissard L, Hoffstetter S, Pernot M. An original technique of brachytherapy in the treatment of epidermoid carcinomas of the buccal mucosa. Int J Radiat Oncol Biol Phys. 1995;33:447–454. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
