

Statins and serum cholesterol's associations with incident dementia and mild cognitive impairment
- PMID: 20841372
- PMCID: PMC3024452
- DOI: 10.1136/jech.2009.100826
Statins and serum cholesterol's associations with incident dementia and mild cognitive impairment
Abstract
Background: Statin use and serum cholesterol reduction have been proposed as preventions for dementia and mild cognitive impairment (MCI).
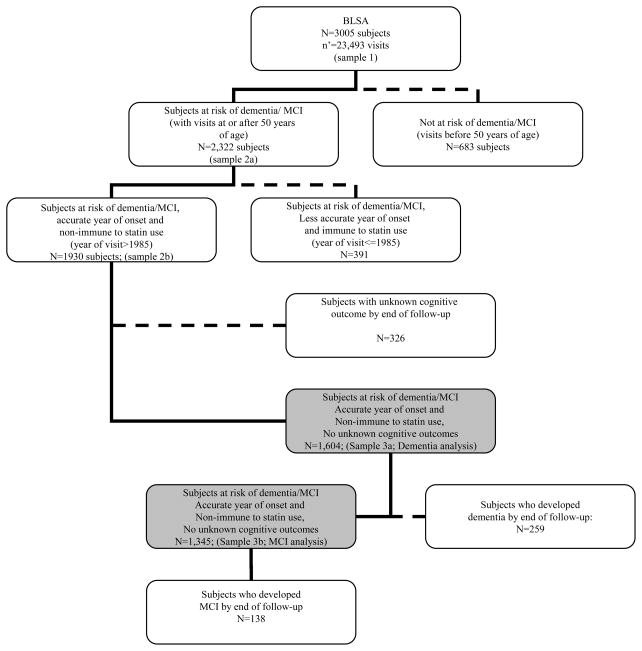
Methods: 1604 and 1345 eligible participants from the Baltimore Longitudinal Study of Aging (BLSA) were followed after age 50 for a median time of around 25 years, to examine the incidence of dementia (n=259) and MCI (n=138), respectively. Statin use (ever-use and time-dependent use), total cholesterol levels (TC; first visit and time-dependent), TC change trajectory from first visit and high-density lipoprotein (HDL-C):TC ratio (first visit and time-dependent) were the main exposures of interest. Cox proportional hazards models were used.
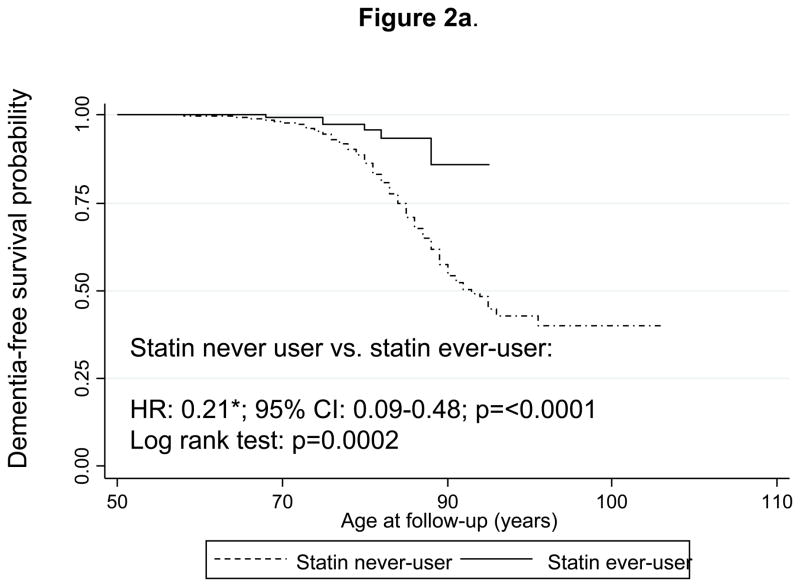
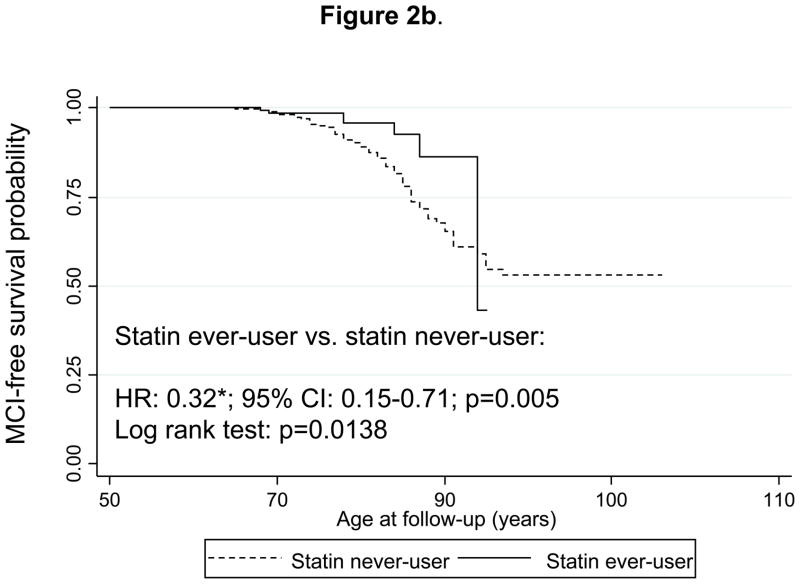
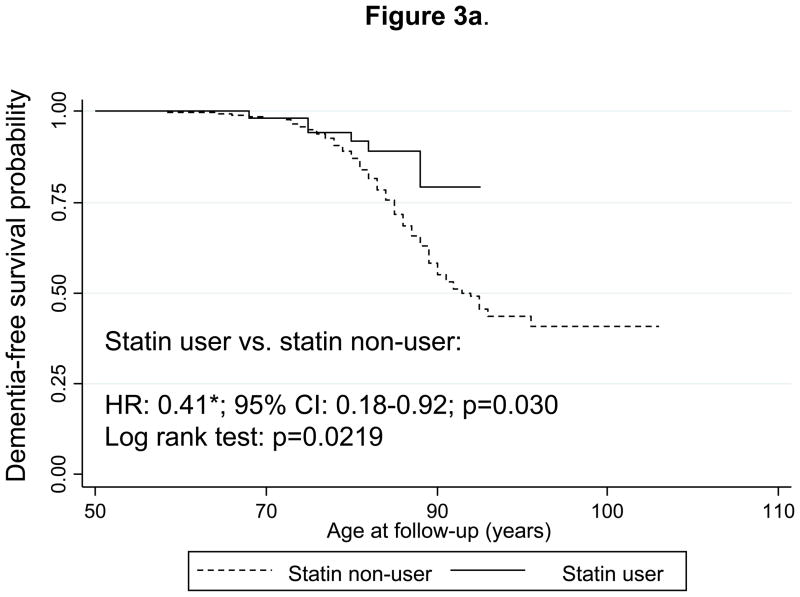
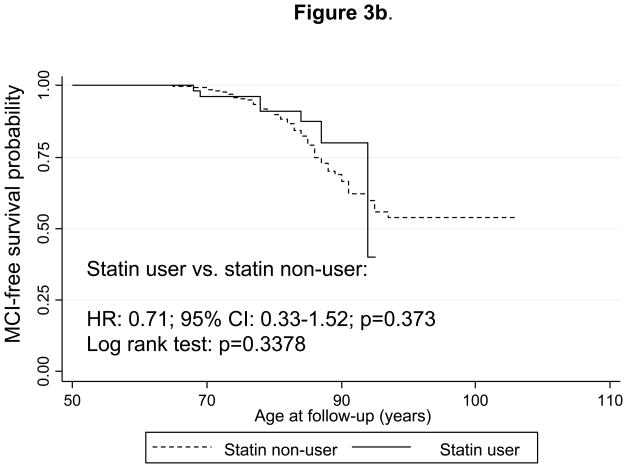
Results: Participants with incident dementia had a higher first-visit TC compared with participants who remained free of dementia and MCI, while first-visit TC was higher among statin ever-users compared with never-users (age-unadjusted associations). Statin users had a two- to threefold lower risk of developing dementia (HR=0.41; 95% CI 0.18 to 0.92), but not MCI, when considering time-dependent 'statin use' with propensity score model adjustment. This association remained significant independently of serum cholesterol exposures. An elevated first-visit TC was associated with reduced MCI risk (upper quartile (Q(4)) vs Q(1): HR=0.51; 95% CI 0.29 to 0.90). Compared with the lowest quartile (Q(1): 0.00-0.19), HDL-C:TC (time-dependent) in (Q(2): 0.19-0.24) was associated with reduced MCI risk (HR=0.58; 95% CI 0.34 to 0.98). Among men only, TC decline from first visit was significantly associated with increased dementia risk (HR=4.21; 95% CI 1.28 to 13.85).
Conclusions: Statins may have multifactorial effects on dementia but not MCI risk. Future interventions may be warranted, and research should focus on optimal serum TC, HDL-C:TC ratio and TC change trajectories.
Conflict of interest statement
COMPETING INTERESTS: None declared.
Figures
References
-
- Hajjar I, Schumpert J, Hirth V, et al. The impact of the use of statins on the prevalence of dementia and the progression of cognitive impairment. J Gerontol A Biol Sci Med Sci. 2002;57:M414–8. - PubMed
-
- Bernick C, Katz R, Smith NL, et al. Statins and cognitive function in the elderly: the Cardiovascular Health Study. Neurology. 2005;65:1388–94. - PubMed
-
- Dufouil C, Richard F, Fievet N, et al. APOE genotype, cholesterol level, lipid-lowering treatment, and dementia: the Three-City Study. Neurology. 2005;64:1531–8. - PubMed
-
- Jick H, Zornberg GL, Jick SS, et al. Statins and the risk of dementia. Lancet. 2000;356:1627–31. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical