

Antiretroviral therapy outcomes of HIV-infected children in the TREAT Asia pediatric HIV observational database
- PMID: 20842043
- PMCID: PMC2975064
- DOI: 10.1097/QAI.0b013e3181f5379a
Antiretroviral therapy outcomes of HIV-infected children in the TREAT Asia pediatric HIV observational database
Abstract
Introduction: We report responses to combination antiretroviral therapy (cART) in the Therapeutics Research, Education, and AIDS Training in Asia Pediatric HIV Observational Database.
Methods: Children included were those who had received cART (ie, ≥3 antiretrovirals) at <18 years. The analysis was intention-to-treat by the first cART regimen. Median values are provided with interquartile ranges; hazard ratios (HRs) with 95% confidence intervals.
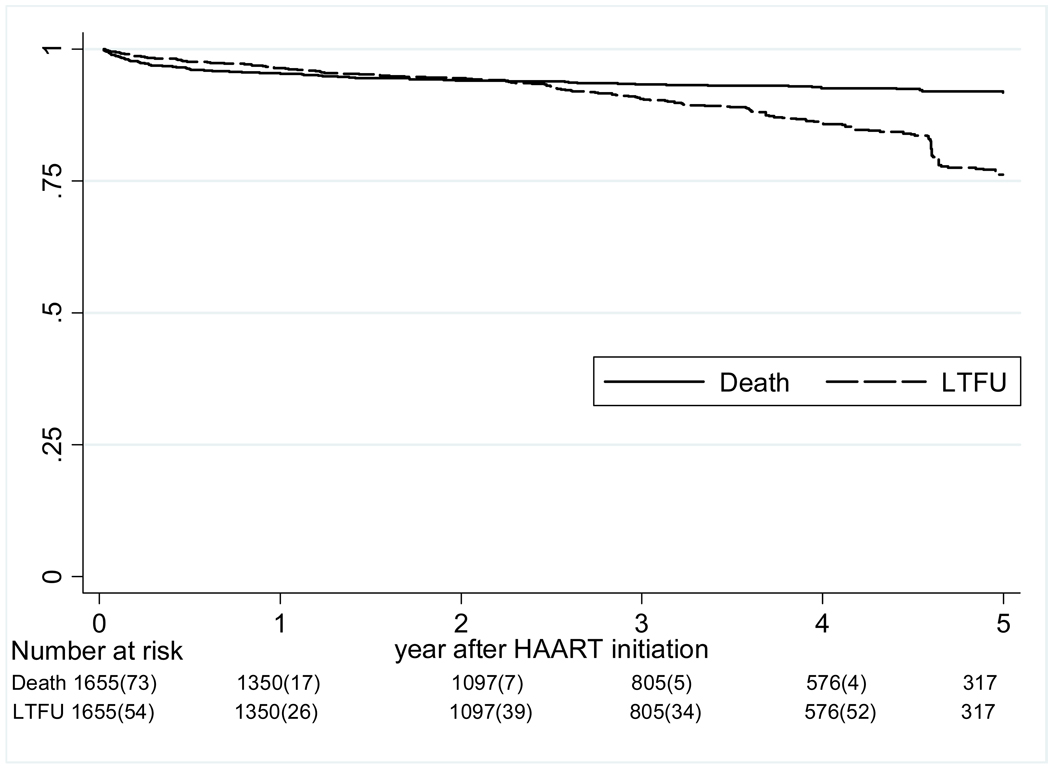
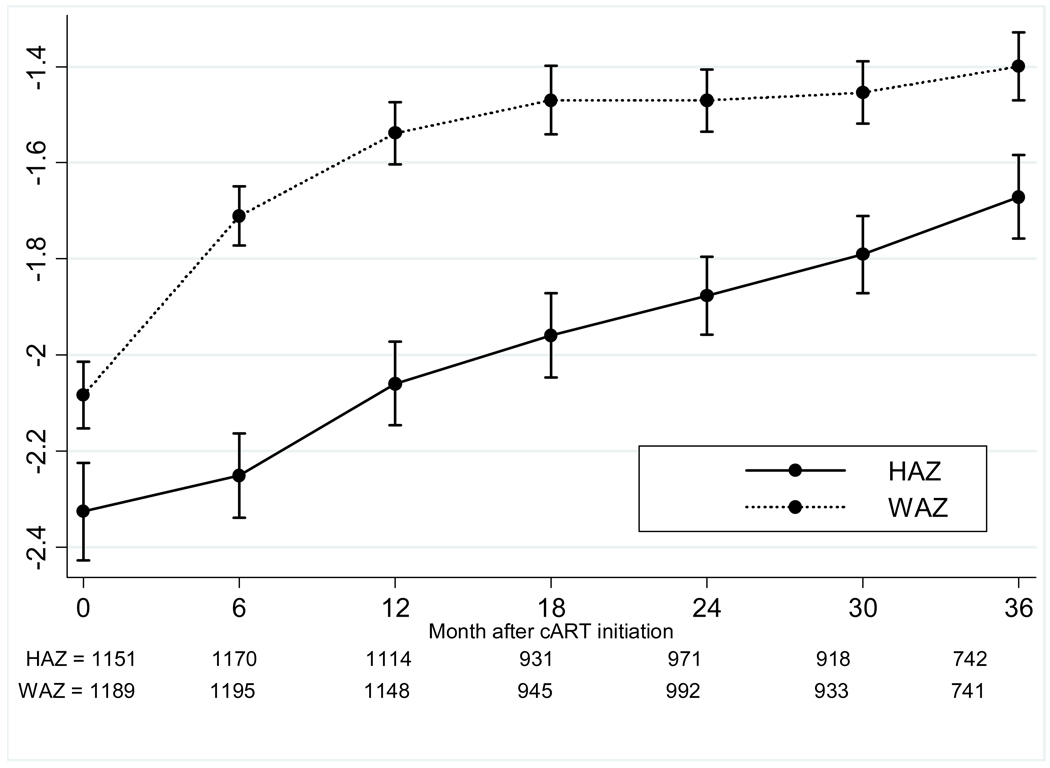
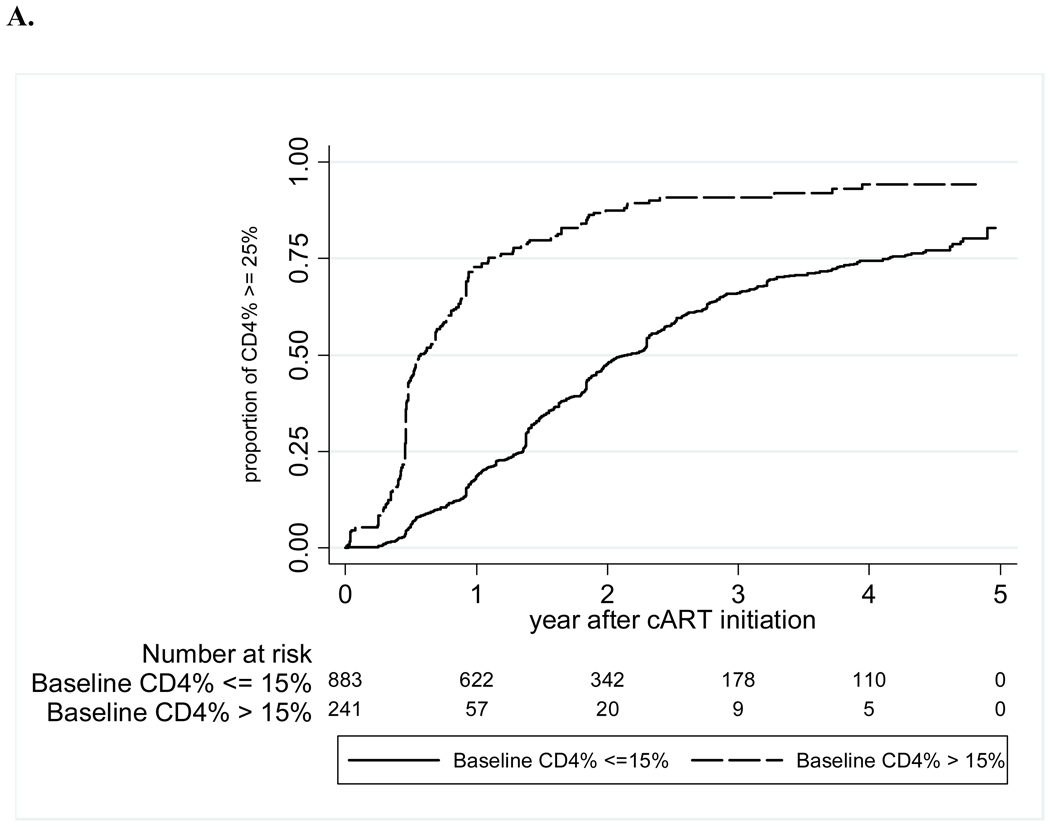
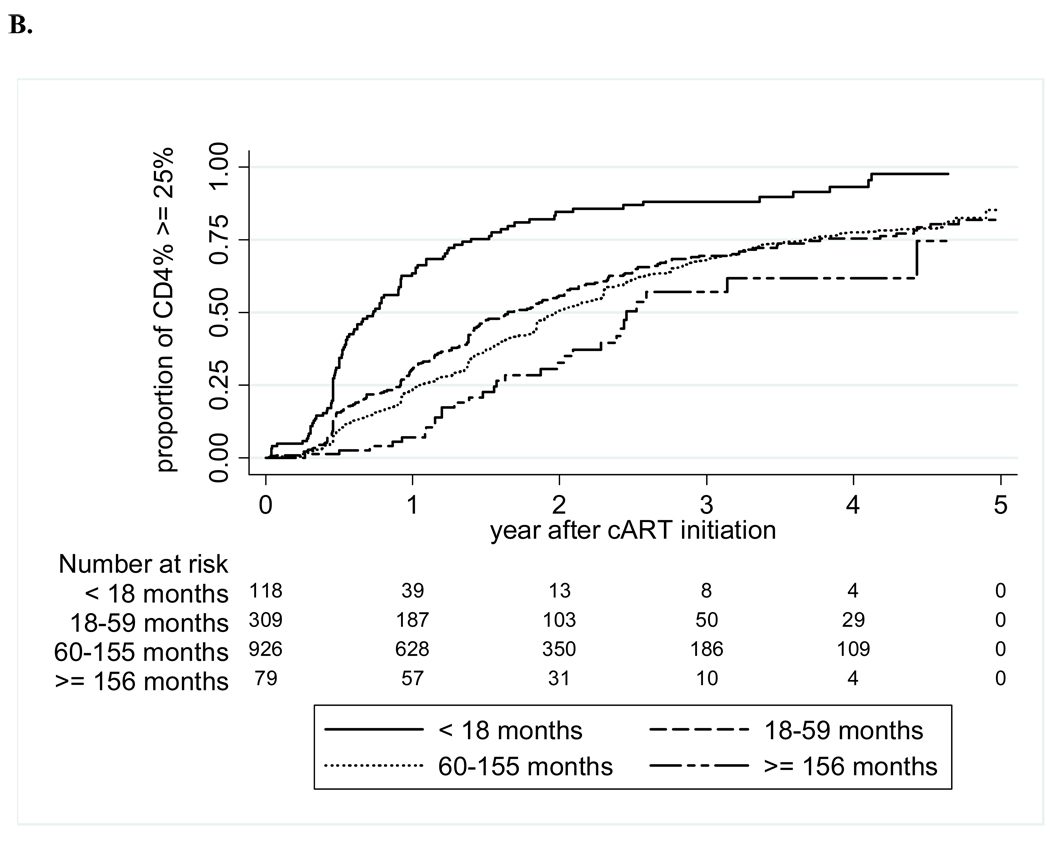
Results: Of the 1655 children included, 50.4% were male, with a median age at cART of 7.0 (3.9-9.8) years and CD4 of 8% (2.0%-15%); 92.5% were started on an NNRTI; median duration of follow-up was 2.9 (1.4-4.6) years. Loss-to-follow-up and death rates were 4.2 (3.7-4.8) and 2.1 (1.7-2.5) per 100 person-years, respectively. At 36 months, median CD4 was 26% (21%-31%); 81% of those with viral load (n = 302) were <400 copies per milliliter. Children who reached CD4 ≥25% within 5 years were more likely to be females (HR: 1.4; 1.2-1.7), start before 18 months old (HR: 3.8; 2.4-6.2), lack a history of monotherapy/dual therapy (HR: 1.7; 1.4-2.5), and have a higher baseline CD4 (per 10% increase: HR: 2; 1.9-2.2).
Conclusions: These data underscore the need for early diagnosis and cART initiation to preserve immune function.
Figures
References
-
- UNAIDS, WHO. AIDS Epidemic Update: December 2009. Geneva: 2009.
-
- UNICEF. Children and AIDS, Fourth stocktaking report. 2009.
-
- WHO. Antiretroviral therapy of HIV infection in infants and children in resource-limited settings: Towards universal access, Recommendations for a public-health approach. 2006. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
