

Hospitalisation for venous thromboembolism in cancer patients and the general population: a population-based cohort study in Denmark, 1997-2006
- PMID: 20842120
- PMCID: PMC2965880
- DOI: 10.1038/sj.bjc.6605883
Hospitalisation for venous thromboembolism in cancer patients and the general population: a population-based cohort study in Denmark, 1997-2006
Abstract
Background: Venous thromboembolism (VTE) frequently complicates cancer. Data on tumour-specific VTE predictors are limited, but may inform strategies to prevent thrombosis.
Methods: We computed incidence rates (IRs) with 95% confidence intervals (CIs) for VTE hospitalisation in a cohort of cancer patients (n=57,591) and in a comparison general-population cohort (n=287,476) in Denmark. The subjects entered the study in 1997-2005, and the follow-up continued through 2006. Using Cox proportional-hazards regression, we estimated relative risks (RRs) for VTE predictors, while adjusting for comorbidity.
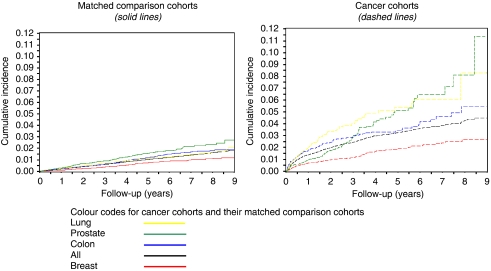
Results: Throughout the follow-up, VTE IR was higher among the cancer patients (IR=8.0, 95% CI=7.6-8.5) than the general population (IR=4.7, 95% CI=4.3-5.1), particularly in the first year after cancer diagnosis (IR=15.0, 95% CI=13.8-16.2, vs IR=8.6, 95% CI=7.6-9.9). Incidence rates of VTE were highest in patients with pancreas (IR=40.9, 95% CI=29.5-56.7), brain (IR=17.7, 95% CI=11.3-27.8) or liver (IR=20.4, 95% CI=9.2-45.3) tumours, multiple myeloma (IR=22.6, 95% CI=15.4-33.2) and among patients with advanced-stage cancers (IR=27.7, 95% CI=24.0-32.0) or those who received chemotherapy or no/symptomatic treatment. The adjusted RR (aRR) for VTE was highest among patients with pancreas (aRR=16.3, 95% CI=8.1-32.6) or brain cancer (aRR=19.8 95% CI=7.1-55.2), multiple myeloma (aRR=46.1, 95% CI=13.1-162.0) and among patients receiving chemotherapy, either alone (aRR=18.5, 95% CI=11.9-28.7) or in combination treatments (aRR=16.2, 95% CI=12.0-21.7).
Conclusions: Risk of VTE is higher among cancer patients than in the general population. Predictors of VTE include recency of cancer diagnosis, cancer site, stage and the type of cancer-directed treatment.
Conflict of interest statement
DPCF, FS, LP, JPF and JAB have no conflicts of interest. KC and JA are employees of Amgen Incorporated. Dr HT Sørensen did not report receiving fees, honoraria, grants or consultancies. Department of Clinical Epidemiology is, however, involved in studies with funding from various other companies as research grants to (and administered by) Aarhus University. None of these other studies have relation with the present study.
Figures
References
-
- Andersen TF, Madsen M, Jorgensen J, Mellemkjoer L, Olsen JH (1999) The danish national hospital register. A valuable source of data for modern health sciences. Dan Med Bull 46(3): 263–268 - PubMed
-
- Arcelus JI, Caprini JA, Monreal M, Suarez C, Gonzalez-Fajardo J (2003) The management and outcome of acute venous thromboembolism: a prospective registry including 4011 patients. J Vasc Surg 38(5): 916–922 - PubMed
-
- Baron JA, Gridley G, Weiderpass E, Nyren O, Linet M (1998) Venous thromboembolism and cancer. Lancet 351(9109): 1077–1080 - PubMed
-
- Bernardi E, Piccioli A, Marchiori A, Girolami B, Prandoni P (2001) Upper extremity deep vein thrombosis: risk factors, diagnosis, and management. Semin Vasc Med 1(1): 105–110 - PubMed
-
- Blom JW, Doggen CJ, Osanto S, Rosendaal FR (2005) Malignancies, prothrombotic mutations, and the risk of venous thrombosis. JAMA 293(6): 715–722 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
