

Rapid testing versus karyotyping in Down's syndrome screening: cost-effectiveness and detection of clinically significant chromosome abnormalities
- PMID: 20842178
- PMCID: PMC3039505
- DOI: 10.1038/ejhg.2010.138
Rapid testing versus karyotyping in Down's syndrome screening: cost-effectiveness and detection of clinically significant chromosome abnormalities
Abstract
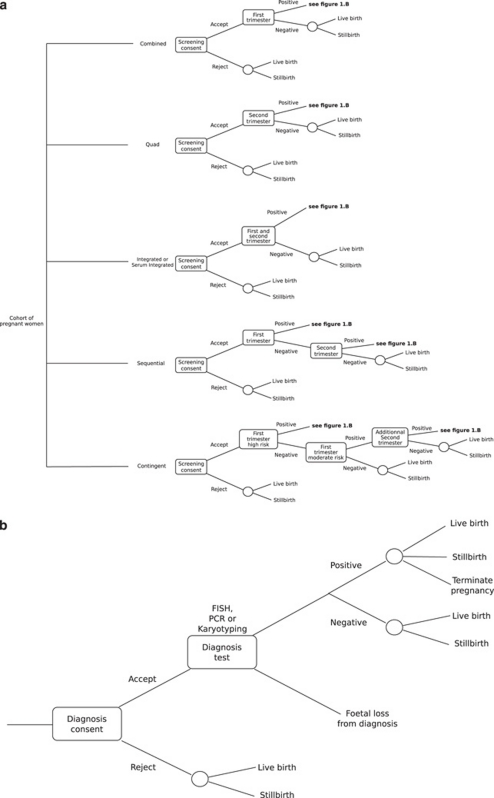
In all, 80% of antenatal karyotypes are generated by Down's syndrome screening programmes (DSSP). After a positive screening, women are offered prenatal foetus karyotyping, the gold standard. Reliable molecular methods for rapid aneuploidy diagnosis (RAD: fluorescence in situ hybridization (FISH) and quantitative fluorescence PCR (QF-PCR)) can detect common aneuploidies, and are faster and less expensive than karyotyping.In the UK, RAD is recommended as a standalone approach in DSSP, whereas the US guidelines recommend that RAD be followed up by karyotyping. A cost-effectiveness (CE) analysis of RAD in various DSSP is lacking. There is a debate over the significance of chromosome abnormalities (CA) detected with karyotyping but not using RAD. Our objectives were to compare the CE of RAD versus karyotyping, to evaluate the clinically significant missed CA and to determine the impact of detecting the missed CA. We performed computer simulations to compare six screening options followed by FISH, PCR or karyotyping using a population of 110948 pregnancies. Among the safer screening strategies, the most cost-effective strategy was contingent screening with QF-PCR (CE ratio of $24084 per Down's syndrome (DS) detected). Using karyotyping, the CE ratio increased to $27898. QF-PCR missed only six clinically significant CA of which only one was expected to confer a high risk of an abnormal outcome. The incremental CE ratio (ICER) to find the CA missed by RAD was $66608 per CA. These costs are much higher than those involved for detecting DS cases. As the DSSP are mainly designed for DS detection, it may be relevant to question the additional costs of karyotyping.
Figures
References
-
- Caine A, Maltby AE, Parkin CA, Waters JJ, Crolla JA. Prenatal detection of Down's syndrome by rapid aneuploidy testing for chromosomes 13, 18, and 21 by FISH or PCR without a full karyotype: a cytogenetic risk assessment. Lancet. 2005;366:123–128. - PubMed
-
- Wald NJ, Hackshaw AK, Watt H. Nuchal translucency and trisomy 18. Prenat Diagn. 1999;19:995–996. - PubMed
-
- Wapner R, Thom E, Simpson JL, et al. First-trimester screening for trisomies 21 and 18. N Engl J Med. 2003;349:1405–1413. - PubMed
-
- NEQAS National External Quality Assessment Scheme in clinical cytogenetics. Annu Rep. 2000.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
