

Superior oblique tucks for apparent inferior oblique overaction and V-pattern strabismus associated with craniosynostosis
- PMID: 20843188
- PMCID: PMC3932310
- DOI: 10.3109/09273972.2010.507613
Superior oblique tucks for apparent inferior oblique overaction and V-pattern strabismus associated with craniosynostosis
Abstract
Introduction: Apparent inferior oblique overaction and apparent superior oblique underaction are common in strabismus associated with craniosynostosis, and in many cases are likely due to excyclotorsion of the globes, with the rectus muscles acting with oblique vectors. We present a patient with craniosynostosis who underwent bilateral superior oblique tucks to specifically address the excyclotorsion of the globes.
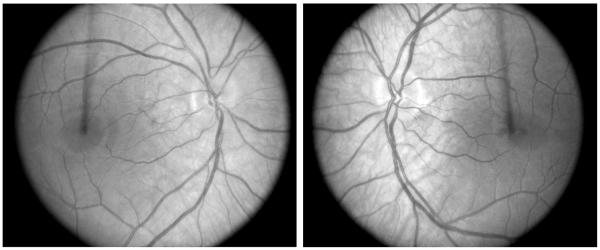
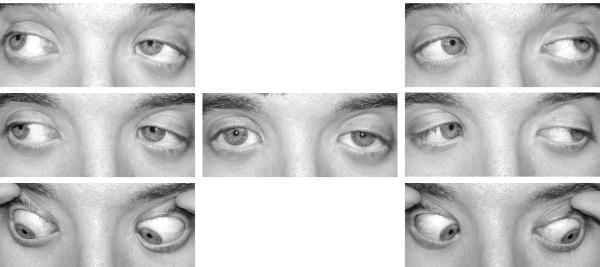
Methods: A 16-year-old male with Saethre-Chotzen syndrome presented with apparent bilateral inferior oblique overaction and apparent bilateral superior oblique underaction. He had 30 prism diopter (PD) esotropia and 5 PD left hypertropia by simultaneous prism and cover test (SPCT) at distance and near fixation. Fundus exam revealed marked excyclotorsion of both globes. The superior oblique tendons were tucked 10 mm bilaterally, using a 6-0 mersilene suture and the medial rectus muscles were recessed 5.5 mm on an adjustable suture with a 10-mm inferior displacement. Surgical results were reviewed at 6 weeks and 2 years postoperatively.
Results: At 6 weeks and 2 years postoperatively, apparent inferior oblique overaction, apparent superior oblique underaction, and V-pattern esotropia were markedly improved. At 2 years, SPCT measurements were 8 PD esotropia in primary position at distance and 4 PD esotropia and 3 PD left dissociated vertical deviation at near.
Conclusions: Bilateral superior oblique tucks are useful in addressing the excyclotorsion that leads to apparent inferior oblique overaction and V-pattern strabismus associated with craniosynostosis.
Figures


Similar articles
-
The Outcome of Inferior Oblique Myectomy for Apparent Inferior Oblique Overaction Associated with Craniosynostosis.Korean J Ophthalmol. 2024 Aug;38(4):296-303. doi: 10.3341/kjo.2023.0146. Epub 2024 Jul 3. Korean J Ophthalmol. 2024. PMID: 38956746 Free PMC article.
-
The efficacy of superior oblique posterior tenectomy in the treatment of A-pattern exotropia without ocular intorsion: A retrospective study.BMC Ophthalmol. 2020 Jan 21;20(1):32. doi: 10.1186/s12886-019-1298-4. BMC Ophthalmol. 2020. PMID: 31964376 Free PMC article.
-
[Long-term clinical effects of the bilateral superior oblique tendon suture spacer in the treatment of A-pattern strabismus].Zhonghua Yan Ke Za Zhi. 2020 Nov 11;56(11):853-858. doi: 10.3760/cma.j.cn112142-20191225-00667. Zhonghua Yan Ke Za Zhi. 2020. PMID: 33152844 Chinese.
-
V-pattern esotropia: a review; and a study of the outcome after bilateral recession of the inferior oblique muscle: a retrospective study of 78 consecutive patients.Binocul Vis Strabismus Q. 2003;18(1):35-48; discussion 49-50. Binocul Vis Strabismus Q. 2003. PMID: 12597768 Review.
-
Uses of the Inferior Oblique Muscle in Strabismus Surgery.Middle East Afr J Ophthalmol. 2015 Jul-Sep;22(3):292-7. doi: 10.4103/0974-9233.159723. Middle East Afr J Ophthalmol. 2015. PMID: 26180466 Free PMC article. Review.
Cited by
-
Ocular manifestations and treatment progress of Crouzon syndrome.Int Ophthalmol. 2024 Sep 5;44(1):367. doi: 10.1007/s10792-024-03293-5. Int Ophthalmol. 2024. PMID: 39235629 Review.
-
Surgical treatment and muscle protein analysis of V-pattern exotropia in craniosynostosis.Sci Rep. 2022 Jul 7;12(1):11524. doi: 10.1038/s41598-022-15707-4. Sci Rep. 2022. PMID: 35798790 Free PMC article.
-
The Outcome of Inferior Oblique Myectomy for Apparent Inferior Oblique Overaction Associated with Craniosynostosis.Korean J Ophthalmol. 2024 Aug;38(4):296-303. doi: 10.3341/kjo.2023.0146. Epub 2024 Jul 3. Korean J Ophthalmol. 2024. PMID: 38956746 Free PMC article.
References
-
- Clark RA, Miller JM, Rosenbaum AL, Demer JL. Heterotopic muscle pulleys or oblique muscle dysfunction? J AAPOS. 1998;2:17–25. - PubMed
-
- Coats DK, Paysse EA, Stager DR. Surgical management of v-pattern strabismus and oblique dysfunction in craniofacial dysostosis. J AAPOS. 2000;4:338–342. - PubMed
-
- Del Monte MA. Special muscle procedures. In: Del Monte MA, Archer SM, editors. Atlas of Pediatric Ophthalmology and Strabismus Surgery. Churchill Livingstone; New York: 1993.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources