

Significant variation in presentation of pulmonary tuberculosis across a high resolution of CD4 strata
- PMID: 20843421
- PMCID: PMC3033769
Significant variation in presentation of pulmonary tuberculosis across a high resolution of CD4 strata
Abstract
Background: The human immunodeficiency virus (HIV) alters the presentation of pulmonary tuberculosis (PTB), but it remains unclear whether alterations occur at a CD4 cell threshold or throughout HIV infection.
Objective: To better understand the relationship between CD4 count and clinical and radiographic presentation of PTB.
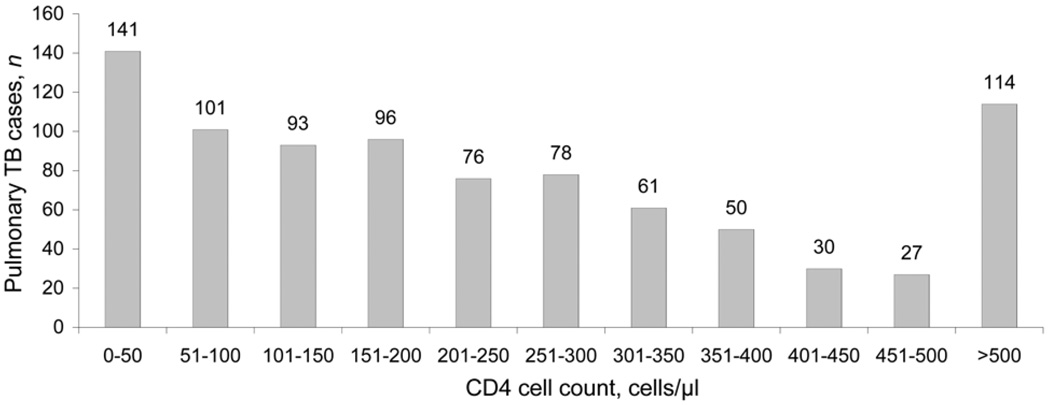
Setting and design: Initial presentations of culture-confirmed PTB patients evaluated at a Ugandan national TB referral center and an affiliated research unit were compared by HIV status and across 11 CD4 cell count strata: 0-50 to >500 cells/μl.
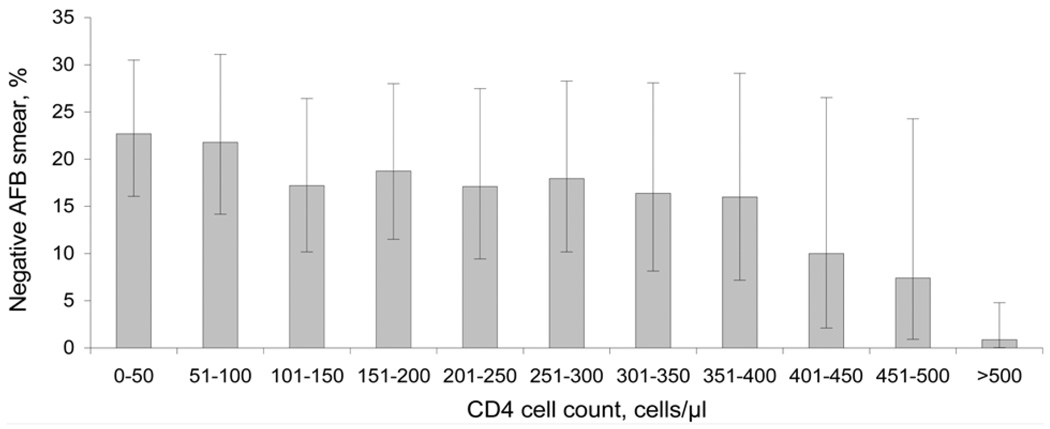
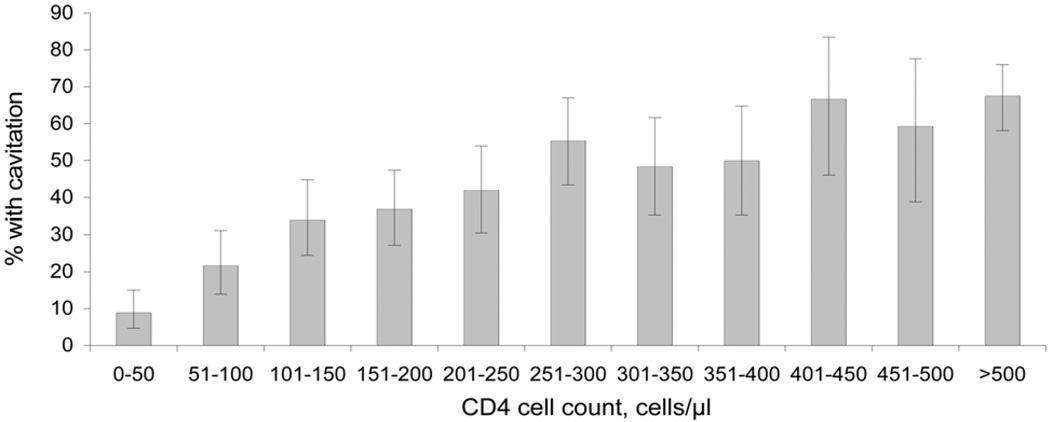
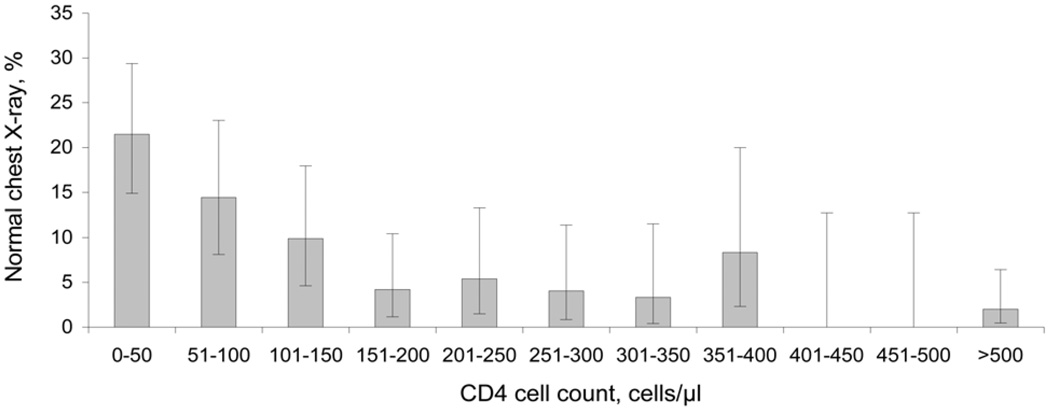
Results: A total of 873 HIV-infected PTB cases were identified. Among HIV-infected PTB cases with CD4 < 50, 21% had a normal chest X-ray (CXR) vs. 2% with CD4 > 500, with a continuous trend across CD4 strata (test for trend, P < 0.001). All radiographic manifestations of PTB displayed significant trends across CD4 strata. HIV-infected vs. non-HIV-infected patients had no significant difference in CXR findings of miliary patterns or pleural effusion at CD4 > 100, normal CXR or fibrosis at CD4 > 150, adenopathy at CD4 > 250, and cavitation or upper lung disease at CD4 > 300. Twenty-three per cent of co-infected cases with CD4 < 50 and 1% with CD4 > 500 had negative acid-fast bacilli (AFB) smears, with a significant trend between (P < 0.001).
Conclusion: Variations in CXR appearance and AFB smear correlate with CD4 decline in significant, continuous trends.
Figures
Comment in
-
Time to rethink guidelines for tuberculosis treatment initiation in HIV-infected patients in developing countries.Int J Tuberc Lung Dis. 2011 Mar;15(3):423-4. Int J Tuberc Lung Dis. 2011. PMID: 21333119 No abstract available.
References
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA. 1999;282:677–686. - PubMed
-
- Ansari NA, Kombe AH, Kenyon TA, et al. Pathology and causes of death in a group of 128 predominantly HIV-positive patients in Botswana, 1997–1998. Int J Tuberc Lung Dis. 2002;6:55–63. - PubMed
-
- Corbett EL, Watt CJ, Walker N, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163:1009–1021. - PubMed
-
- Rana FS, Hawken MP, Mwachari C, et al. Autopsy study of HIV-1-positive and HIV-1-negative adult medical patients in Nairobi, Kenya. J Acquir Immune Defic Syndr. 2000;24:23–29. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
