

Paracetamol use in early life and asthma: prospective birth cohort study
- PMID: 20843914
- PMCID: PMC2939956
- DOI: 10.1136/bmj.c4616
Paracetamol use in early life and asthma: prospective birth cohort study
Abstract
Objective: To determine if use of paracetamol in early life is an independent risk factor for childhood asthma.
Design: Prospective birth cohort study.
Setting: Melbourne Atopy Cohort Study.
Participants: 620 children with a family history of allergic disease, with paracetamol use prospectively documented on 18 occasions from birth to 2 years of age, followed until age 7 years.
Main outcome measures: The primary outcome was childhood asthma, ascertained by questionnaire at 6 and 7 years. Secondary outcomes were infantile wheeze, allergic rhinitis, eczema, and skin prick test positivity.
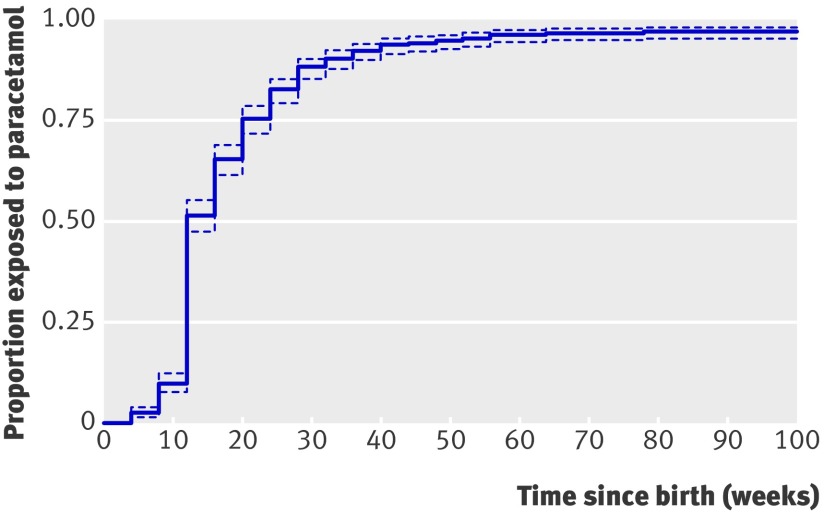
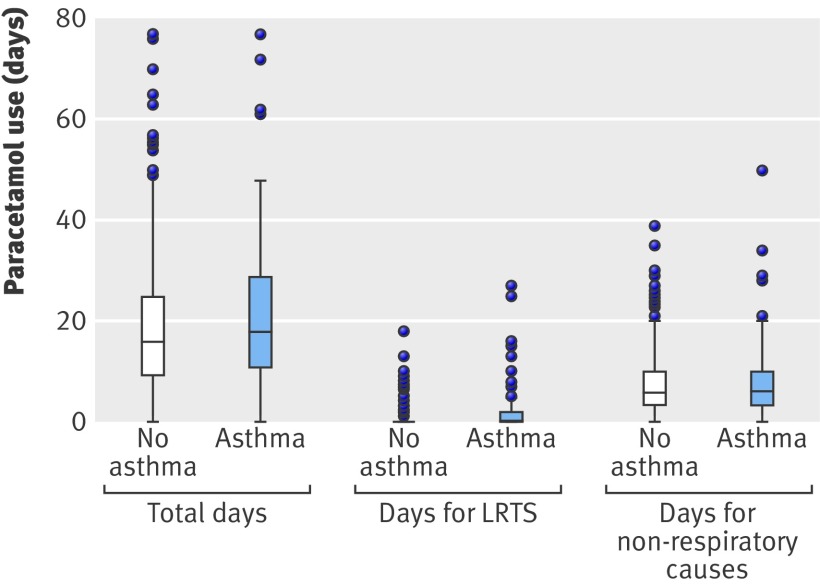
Results: Paracetamol had been used in 51% (295/575) of children by 12 weeks of age and in 97% (556/575) by 2 years. Between 6 and 7 years, 80% (495/620) were followed up; 30% (148) had current asthma. Increasing frequency of paracetamol use was weakly associated with increased risk of childhood asthma (crude odds ratio 1.18, 95% confidence interval 1.00 to 1.39, per doubling of days of use). However, after adjustment for frequency of respiratory infections, this association essentially disappeared (odds ratio 1.08, 0.91 to 1.29). Paracetamol use for non-respiratory causes was not associated with asthma (crude odds ratio 0.95, 0.81 to 1.12).
Conclusions: In children with a family history of allergic diseases, no association was found between early paracetamol use and risk of subsequent allergic disease after adjustment for respiratory infections or when paracetamol use was restricted to non-respiratory tract infections. These findings suggest that early paracetamol use does not increase the risk of asthma.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Kogan MD, Pappas G, Yu SM, Kotelchuck M. Over-the-counter medication use among US preschool-age children. JAMA 1994;272:1025-30. - PubMed
-
- Eneli I, Sadri K, Camargo C Jr, Barr RG. Acetaminophen and the risk of asthma: the epidemiologic and pathophysiologic evidence. Chest 2005;127:604-12. - PubMed
-
- McKeever TM, Lewis SA, Smit HA, Burney P, Britton JR, Cassano PA. The association of acetaminophen, aspirin, and ibuprofen with respiratory disease and lung function. Am J Respir Crit Care Med 2005;171:966-71. - PubMed
-
- Barr RG, Wentowski CC, Curhan GC, Somers SC, Stampfer MJ, Schwartz J, et al. Prospective study of acetaminophen use and newly diagnosed asthma among women. Am J Respir Crit Care Med 2004;169:836-41. - PubMed
-
- Lesko SM, Louik C, Vezina RM, Mitchell AA. Asthma morbidity after the short-term use of ibuprofen in children. Pediatrics 2002;109:E20. - PubMed