

Prostate specific antigen concentration at age 60 and death or metastasis from prostate cancer: case-control study
- PMID: 20843935
- PMCID: PMC2939950
- DOI: 10.1136/bmj.c4521
Prostate specific antigen concentration at age 60 and death or metastasis from prostate cancer: case-control study
Abstract
Objective: To determine the relation between concentrations of prostate specific antigen at age 60 and subsequent diagnosis of clinically relevant prostate cancer in an unscreened population to evaluate whether screening for prostate cancer and chemoprevention could be stratified by risk.
Design: Case-control study with 1:3 matching nested within a highly representative population based cohort study.
Setting: General population of Sweden taking part in the Malmo Preventive Project. Cancer registry at the National Board of Health and Welfare.
Participants: 1167 men aged 60 who provided blood samples in 1981 and were followed up to age 85.
Main outcome measures: Metastasis or death from prostate cancer.
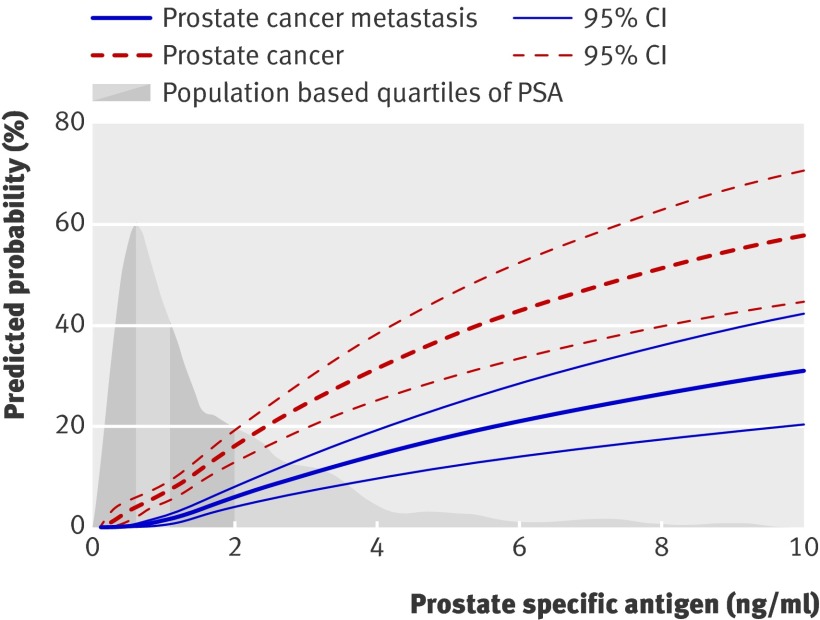
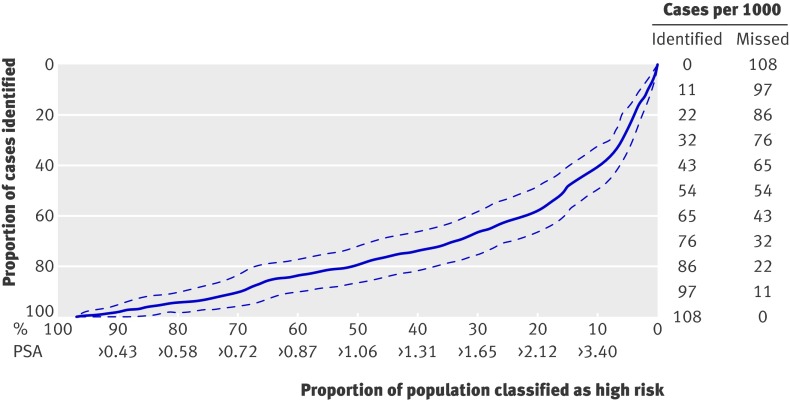
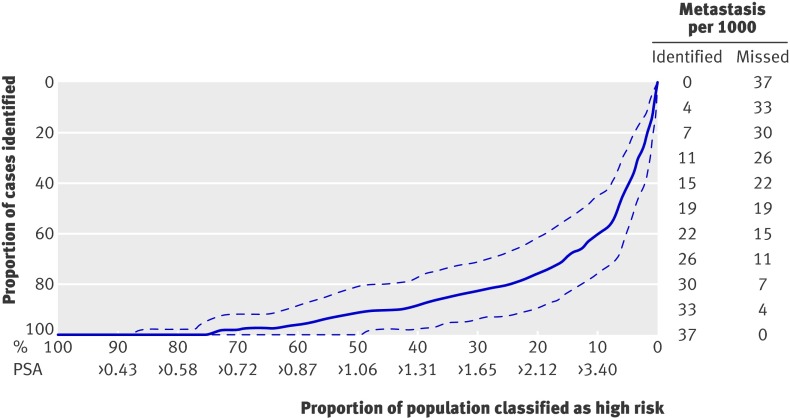
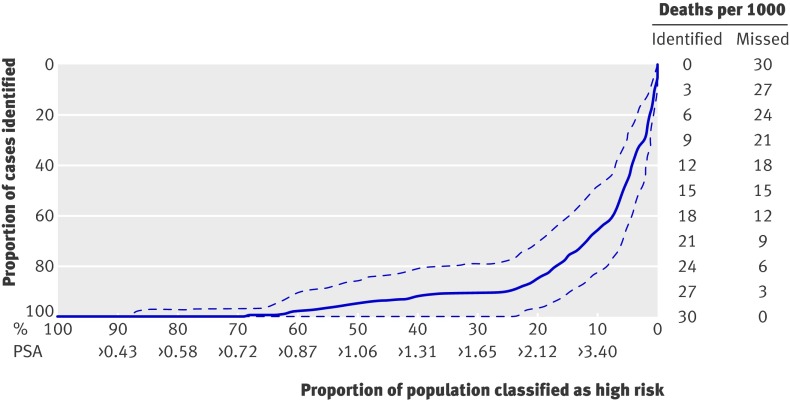
Results: The rate of screening during the course of the study was low. There were 43 cases of metastasis and 35 deaths from prostate cancer. Concentration of prostate specific antigen at age 60 was associated with prostate cancer metastasis (area under the curve 0.86, 95% confidence interval 0.79 to 0.92; P<0.001) and death from prostate cancer (0.90, 0.84 to 0.96; P<0.001). The greater the number for the area under the curve (values from 0 to 1) the better the test. Although only a minority of the men with concentrations in the top quarter (>2 ng/ml) develop fatal prostate cancer, 90% (78% to 100%) of deaths from prostate cancer occurred in these men. Conversely, men aged 60 with concentrations at the median or lower (≤1 ng/ml) were unlikely to have clinically relevant prostate cancer (0.5% risk of metastasis by age 85 and 0.2% risk of death from prostate cancer).
Conclusions: The concentration of prostate specific antigen at age 60 predicts lifetime risk of metastasis and death from prostate cancer. Though men aged 60 with concentrations below the median (≤1 ng/ml) might harbour prostate cancer, it is unlikely to become life threatening. Such men could be exempted from further screening, which should instead focus on men with higher concentrations.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
Comment in
-
Prostate cancer: Risk stratification of PSA-based screening.Nat Rev Urol. 2010 Dec;7(12):643. doi: 10.1038/nrurol.2010.192. Nat Rev Urol. 2010. PMID: 21188769 No abstract available.
-
Words of Wisdom. Re: prostate specific antigen concentration at age 60 and death or metastasis from prostate cancer: case-control study.Eur Urol. 2011 Feb;59(2):304-5. doi: 10.1016/j.eururo.2010.11.012. Eur Urol. 2011. PMID: 21414880 No abstract available.
-
Re.: Prostate specific antigen concentration at age 60 and death or metastasis from prostate cancer: case-control study.J Urol. 2011 May;185(5):1705. doi: 10.1016/S0022-5347(11)60222-X. J Urol. 2011. PMID: 22088695 No abstract available.
References
-
- Schroder FH, Hugosson J, Roobol MJ, Tammela TL, Ciatto S, Nelen V, et al. Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 2009;360:1320-8. - PubMed
-
- Ross LE, Berkowitz Z, Ekwueme DU. Use of the prostate-specific antigen test among U.S. men: findings from the 2005 National Health Interview Survey. Cancer Epidemiol Biomarkers Prev 2008;17:636-44. - PubMed
-
- Thompson IM, Ankerst DP, Chi C, Goodman PJ, Tangen CM, Lucia MS, et al. Assessing prostate cancer risk: results from the Prostate Cancer Prevention Trial. J Natl Cancer Inst 2006;98:529-34. - PubMed
-
- Hernandez J, Thompson IM. Prostate-specific antigen: a review of the validation of the most commonly used cancer biomarker. Cancer 2004;101:894-904. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical