

Autologous chondrocyte implantation: a systematic review
- PMID: 20844166
- PMCID: PMC7373451
- DOI: 10.2106/JBJS.J.00049
Autologous chondrocyte implantation: a systematic review
Abstract
Background: The purpose of the present study was to determine (1) whether the current literature supports the choice of using autologous chondrocyte implantation over other cartilage procedures with regard to clinical outcome, magnetic resonance imaging, arthroscopic assessment, and durability of treatment, (2) whether the current literature supports the use of a specific generation of autologous chondrocyte implantation, and (3) whether there are patient-specific and defect-specific factors that influence outcomes after autologous chondrocyte implantation in comparison with other cartilage repair or restoration procedures.
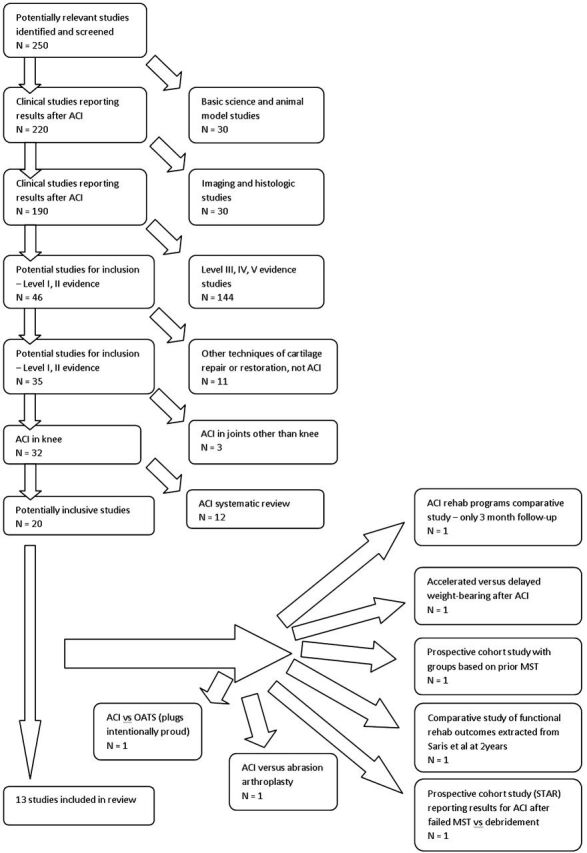
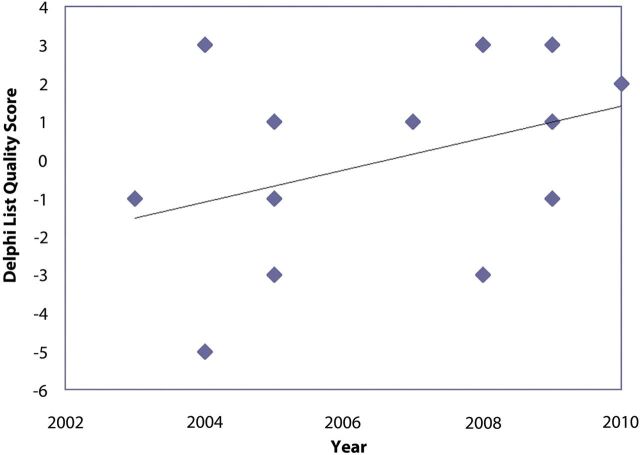
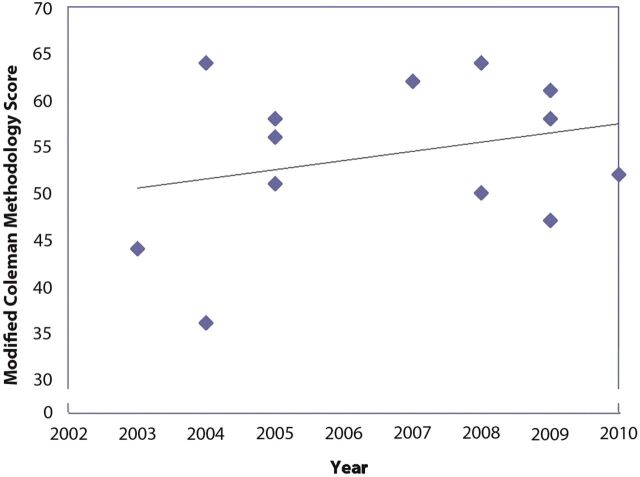
Methods: We conducted a systematic review of multiple databases in which we evaluated Level-I and II studies comparing autologous chondrocyte implantation with another cartilage repair or restoration technique as well as comparative intergenerational studies of autologous chondrocyte implantation. The methodological quality of studies was evaluated with use of Delphi list and modified Coleman methodology scores. Effect size analysis was performed for all outcome measures.
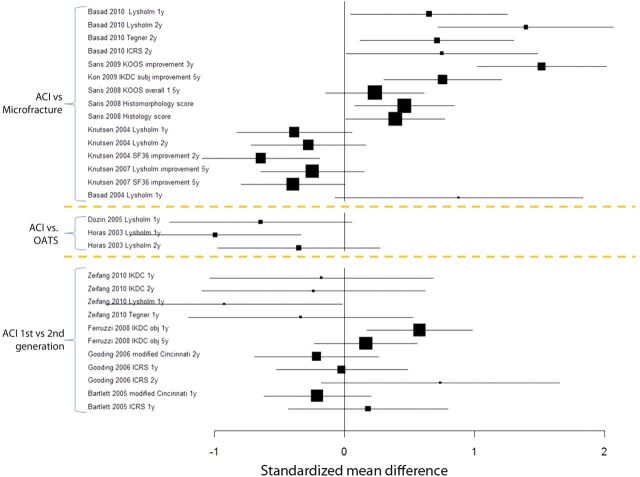
Results: Thirteen studies (917 subjects) were included. Study methodological quality improved with later publication dates. The mean modified Coleman methodology score was 54 (of 100). Patients underwent autologous chondrocyte implantation (n = 604), microfracture (n = 271), or osteochondral autograft (n = 42). All surgical techniques demonstrated improvement in comparison with the preoperative status. Three of seven studies showed better clinical outcomes after autologous chondrocyte implantation in comparison with microfracture after one to three years of follow-up, whereas one study showed better outcomes two years after microfracture and three other studies showed no difference in these treatments after one to five years. Clinical outcomes after microfracture deteriorated after eighteen to twenty-four months (in three of seven studies). Autologous chondrocyte implantation and osteochondral autograft demonstrated equivalent short-term clinical outcomes, although there was more rapid improvement after osteochondral autograft (two studies). Although outcomes were equivalent between first and second-generation autologous chondrocyte implantation and between open and arthroscopic autologous chondrocyte implantation, complication rates were higher with open, periosteal-cover, first-generation autologous chondrocyte implantation (four studies). Younger patients with a shorter preoperative duration of symptoms and fewer prior surgical procedures had the best outcomes after both autologous chondrocyte implantation and microfracture. A defect size of >4 cm(2) was the only factor predictive of better outcomes when autologous chondrocyte implantation was compared with a non-autologous chondrocyte implantation surgical technique.
Conclusions: Cartilage repair or restoration in the knee provides short-term success with microfracture, autologous chondrocyte implantation, or osteochondral autograft. There are patient-specific and defect-specific factors that influence clinical outcomes.
Figures
References
-
- Buckwalter J Mankin H. Articular cartilage. Part II: degeneration and osteoarthrosis, repair, regeneration, and transplantation. J Bone Joint Surg Am. 1997;79:612-32.
-
- Alford JW Cole BJ. Cartilage restoration, part 1: basic science, historical perspective, patient evaluation, and treatment options. Am J Sports Med. 2005;33:295-306. - PubMed
-
- Heir S Nerhus TK Røtterud JH Løken S Ekeland A Engebretsen L Arøen A. Focal cartilage defects in the knee impair quality of life as much as severe osteoarthritis: a comparison of knee injury and osteoarthritis outcome score in 4 patient categories scheduled for knee surgery. Am J Sports Med. 2010;38:231-7. - PubMed
-
- Steadman JR Rodkey WG Briggs KK. Microfracture to treat full-thickness chondral defects: surgical technique, rehabilitation, and outcomes. J Knee Surg. 2002;15:170-6. - PubMed
-
- Saris DB Vanlauwe J Victor J Almqvist KF Verdonk R Bellemans J Luyten FP; TIG/ACT/01/2000&EXT Study Group. Treatment of symptomatic cartilage defects of the knee: characterized chondrocyte implantation results in better clinical outcome at 36 months in a randomized trial compared to microfracture. Am J Sports Med. 2009;37 Suppl 1:10S-9S. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
