

Assessing the performance of a computer-based policy model of HIV and AIDS
- PMID: 20844741
- PMCID: PMC2936574
- DOI: 10.1371/journal.pone.0012647
Assessing the performance of a computer-based policy model of HIV and AIDS
Abstract
Background: Model-based analyses, conducted within a decision analytic framework, provide a systematic way to combine information about the natural history of disease and effectiveness of clinical management strategies with demographic and epidemiological characteristics of the population. Among the challenges with disease-specific modeling include the need to identify influential assumptions and to assess the face validity and internal consistency of the model.
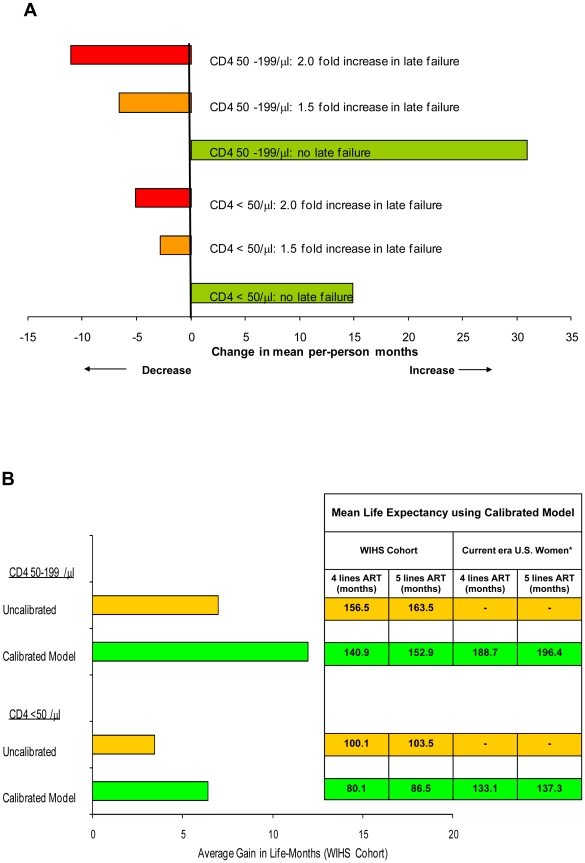
Methods and findings: We describe a series of exercises involved in adapting a computer-based simulation model of HIV disease to the Women's Interagency HIV Study (WIHS) cohort and assess model performance as we re-parameterized the model to address policy questions in the U.S. relevant to HIV-infected women using data from the WIHS. Empiric calibration targets included 24-month survival curves stratified by treatment status and CD4 cell count. The most influential assumptions in untreated women included chronic HIV-associated mortality following an opportunistic infection, and in treated women, the 'clinical effectiveness' of HAART and the ability of HAART to prevent HIV complications independent of virologic suppression. Good-fitting parameter sets required reductions in the clinical effectiveness of 1st and 2nd line HAART and improvements in 3rd and 4th line regimens. Projected rates of treatment regimen switching using the calibrated cohort-specific model closely approximated independent analyses published using data from the WIHS.
Conclusions: The model demonstrated good internal consistency and face validity, and supported cohort heterogeneities that have been reported in the literature. Iterative assessment of model performance can provide information about the relative influence of uncertain assumptions and provide insight into heterogeneities within and between cohorts. Description of calibration exercises can enhance the transparency of disease-specific models.
Conflict of interest statement
Figures


References
-
- Carpenter CC, Cooper DA, Fischl MA, Gatell JM, Gazzard BG, et al. Antiretroviral therapy in adults: updated recommendations of the International AIDS Society-USA Panel. JAMA. 2000;283:381–390. - PubMed
-
- Detels R, Muñoz A, McFarlane G, Kingsley LA, Margolick JB, et al. Effectiveness of potent antiretroviral therapy on time to AIDS and death in men with known HIV infection duration. Multicenter AIDS Cohort Study Investigators. JAMA. 1998;280:1497–1503. - PubMed
-
- Detels R, Tarwater P, Phair JP, Margolick J, Riddler SA, et al. Effectiveness of potent antiretroviral therapies on the incidence of opportunistic infections before and after AIDS diagnosis. AIDS. 2001;15:347–355. - PubMed
-
- Yamashita TE, Phair JP, Muñoz A, Margolick JB, Detels R, et al. Immunologic and virologic response to highly active antiretroviral therapy in the Multicenter AIDS Cohort Study. AIDS. 2001;15:735–746. - PubMed
-
- Yeni PG, Hammer SM, Carpenter CC, Cooper DA, Fischl MA, et al. Antiretroviral treatment for adult HIV infection in 2002: updated recommendations of the International AIDS Society-USA Panel. JAMA. 2002;288:222–235. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
