

Hip offset in total hip arthroplasty: quantitative measurement with navigation
- PMID: 20844997
- PMCID: PMC3018189
- DOI: 10.1007/s11999-010-1554-7
Hip offset in total hip arthroplasty: quantitative measurement with navigation
Abstract
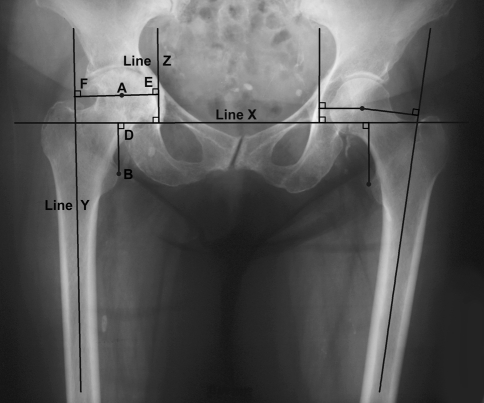
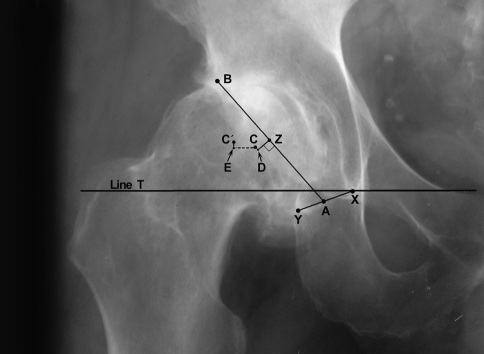
Background: Offset in THA correlates to abductor muscle function, wear, and impingement. Femoral offset after THA is not independent of the cup center of rotation (COR) so hip offset, a combination of femoral offset and change in hip COR, becomes the important measurement.
Questions/purposes: We therefore asked whether hip offset in arthritic hips would correlate with cup COR; whether offset could always be balanced within 6 mm of contralateral normal hips; and whether hip length could also be kept within 6 mm.
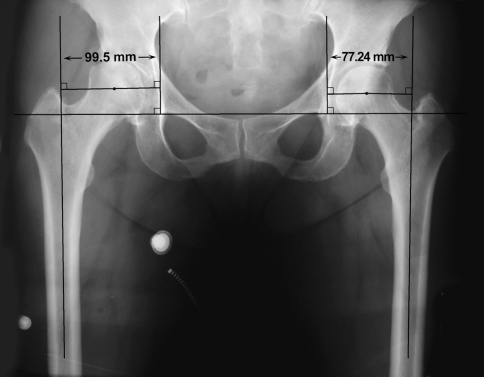
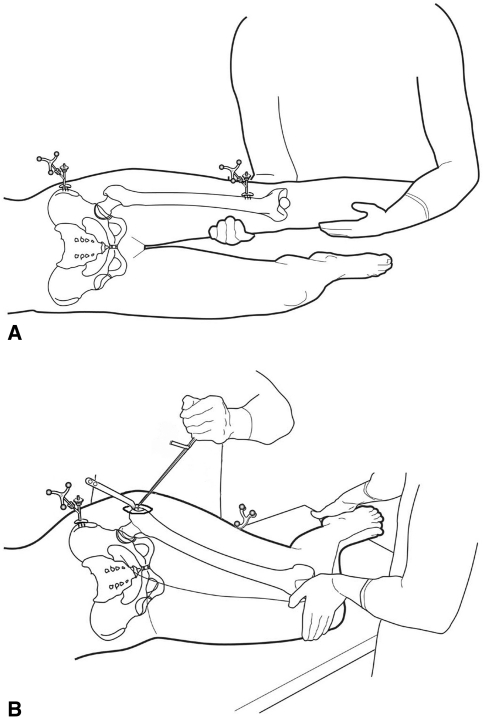
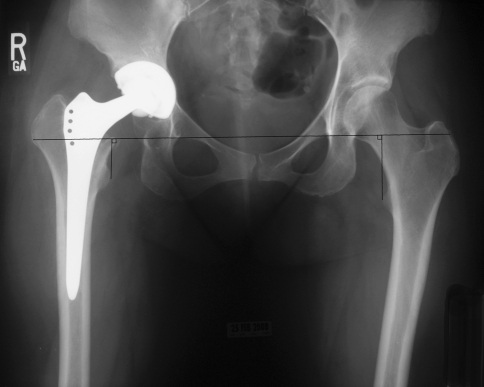
Methods: We compared hip offset of arthritic and contralateral normal hips on radiographs in 82 patients (82 hips) who had THA. We used computer navigation in all patients with the aim of reconstructing the hip offset and to compare hip offset change to the quantitative change of the hip COR.
Results: The preoperative radiographic change to equalize the offset ranged from -12 to +21 mm (mean, 1.5); postoperatively the change was 1.4 ± 6.4 mm and was within ± 6 mm in 78 of 82 hips. As COR displaced superiorly from 3 to 6+ mm the offset had to be substantially increased. Only with COR 0-3 mm superior and 0-5 mm medial was offset always within 5 mm.
Conclusions: Hip offset reconstruction was directly related to the position of the hip COR, and navigation allowed quantitative control of offset and hip length.
Figures


References
-
- Charles MN, Bourne RB, Davey JR, Greenwald AS, Morrey BF, Rorabeck CH. Soft-tissue balancing of the hip: the role of femoral offset restoration. J Bone Joint Surg Am. 2004;86:1078–1088. - PubMed
-
- Dolhain P, Tsigaras H, Bourne RB, Rorabeck CH, Mac Donald S, Mc Calden R. The effectiveness of dual offset stems in restoring offset during total hip replacement. Acta Orthop Belg. 2002;68:490–499. - PubMed
-
- Dorr LD. Hip Arthroplasty: Minimally Invasive Techniques and Computer Navigation. 1. Philadelphia, PA: WB Saunders; 2005.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
