

Practice effects in healthy adults: a longitudinal study on frequent repetitive cognitive testing
- PMID: 20846444
- PMCID: PMC2955045
- DOI: 10.1186/1471-2202-11-118
Practice effects in healthy adults: a longitudinal study on frequent repetitive cognitive testing
Abstract
Background: Cognitive deterioration is a core symptom of many neuropsychiatric disorders and target of increasing significance for novel treatment strategies. Hence, its reliable capture in long-term follow-up studies is prerequisite for recording the natural course of diseases and for estimating potential benefits of therapeutic interventions. Since repeated neuropsychological testing is required for respective longitudinal study designs, occurrence, time pattern and magnitude of practice effects on cognition have to be understood first under healthy good-performance conditions to enable design optimization and result interpretation in disease trials.
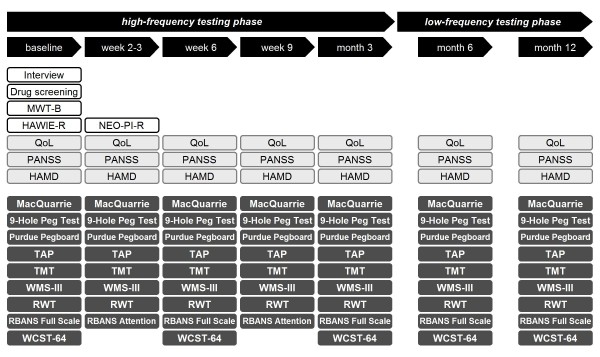
Methods: Healthy adults (N = 36; 47.3 ± 12.0 years; mean IQ 127.0 ± 14.1; 58% males) completed 7 testing sessions, distributed asymmetrically from high to low frequency, over 1 year (baseline, weeks 2-3, 6, 9, months 3, 6, 12). The neuropsychological test battery covered 6 major cognitive domains by several well-established tests each.
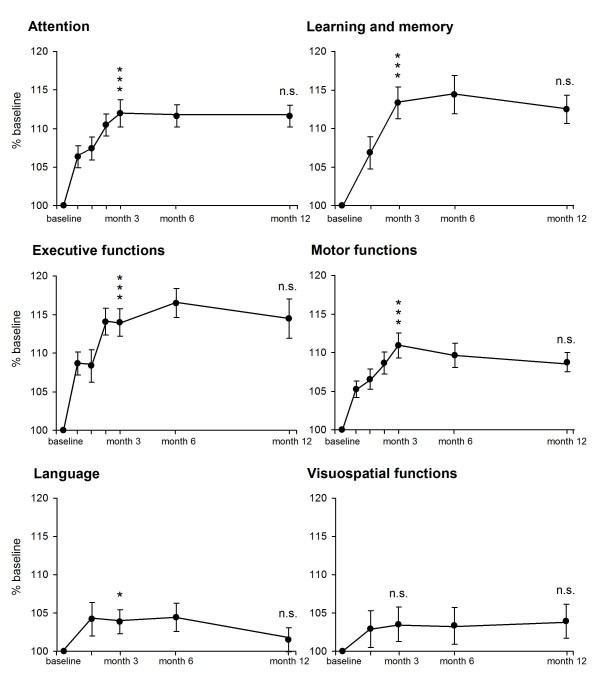
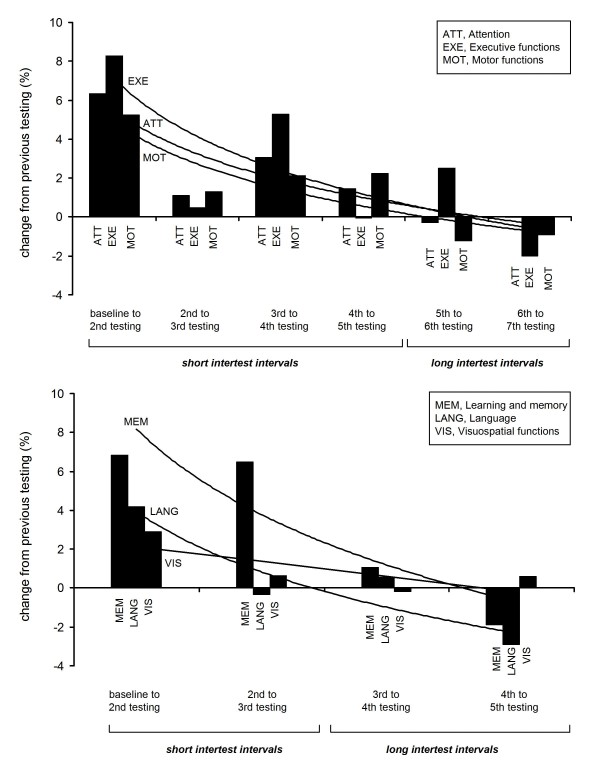
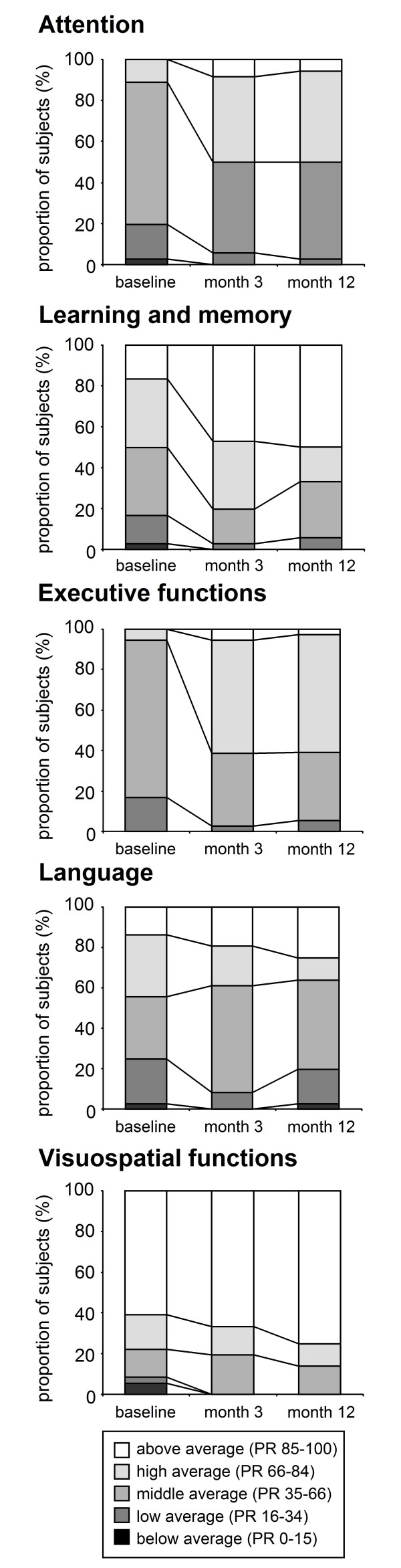
Results: Most tests exhibited a similar pattern upon repetition: (1) Clinically relevant practice effects during high-frequency testing until month 3 (Cohen's d 0.36-1.19), most pronounced early on, and (2) a performance plateau thereafter upon low-frequency testing. Few tests were non-susceptible to practice or limited by ceiling effects. Influence of confounding variables (age, IQ, personality) was minor.
Conclusions: Practice effects are prominent particularly in the early phase of high-frequency repetitive cognitive testing of healthy well-performing subjects. An optimal combination and timing of tests, as extractable from this study, will aid in controlling their impact. Moreover, normative data for serial testing may now be collected to assess normal learning curves as important comparative readout of pathological cognitive processes.
Figures
References
-
- Green MF. What are the functional consequences of neurocognitive deficits in schizophrenia? Am J Psychiatry. 1996;153:321–330. - PubMed
-
- Farias ST, Harrell E, Neumann C, Houtz A. The relationship between neuropsychological performance and daily functioning in individuals with Alzheimer's disease: ecological validity of neuropsychological tests. Arch Clin Neuropsychol. 2003;18:655–672. - PubMed
-
- McCaffrey RJ, Duff K, Westervelt HJ. Practitioner's guide to evaluating change with neuropsychological assessment instruments. New York: Kluwer Academic/Plenum Publishers; 2000.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
