

Late gadolinium-enhancement cardiac magnetic resonance identifies postinfarction myocardial fibrosis and the border zone at the near cellular level in ex vivo rat heart
- PMID: 20847191
- PMCID: PMC3398602
- DOI: 10.1161/CIRCIMAGING.108.835793
Late gadolinium-enhancement cardiac magnetic resonance identifies postinfarction myocardial fibrosis and the border zone at the near cellular level in ex vivo rat heart
Abstract
Background: using a resolution 1000-fold higher than prior studies, we studied (1) the degree to which late gadolinium-enhancement (LGE) cardiac magnetic resonance tracks fibrosis from chronic myocardial infarction and (2) the relationship between intermediate signal intensity and partial volume averaging at distinct "smooth" infarct borders versus disorganized mixtures of fibrosis and viable cardiomyocytes.
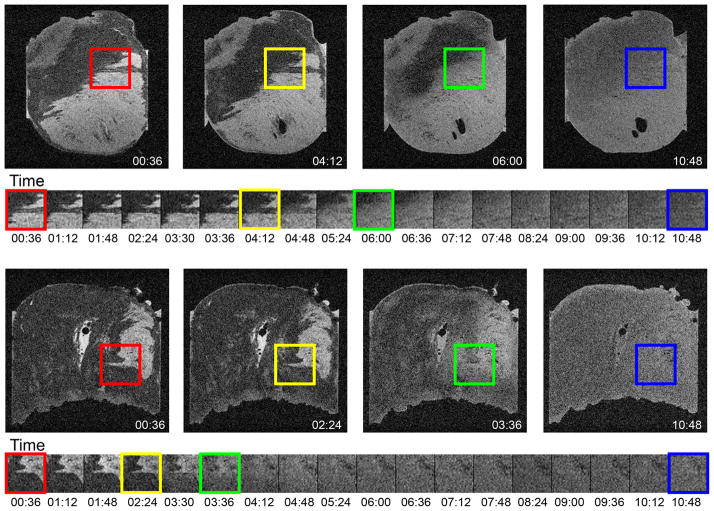
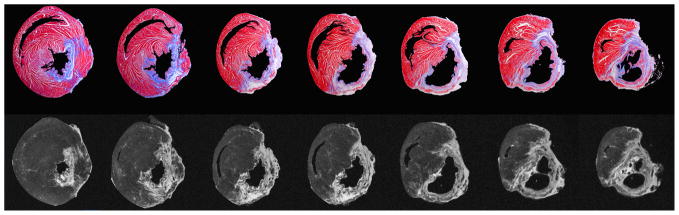
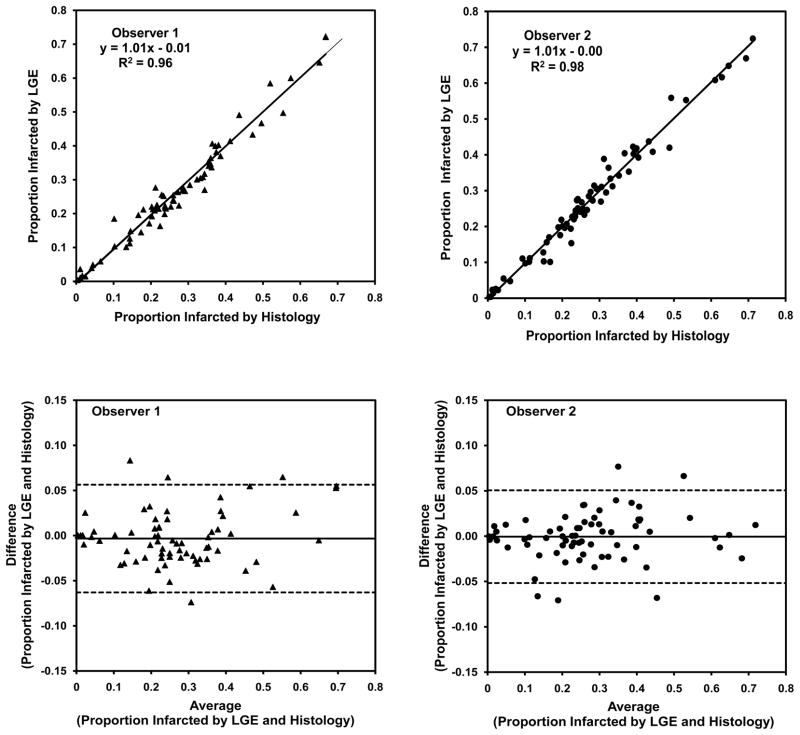
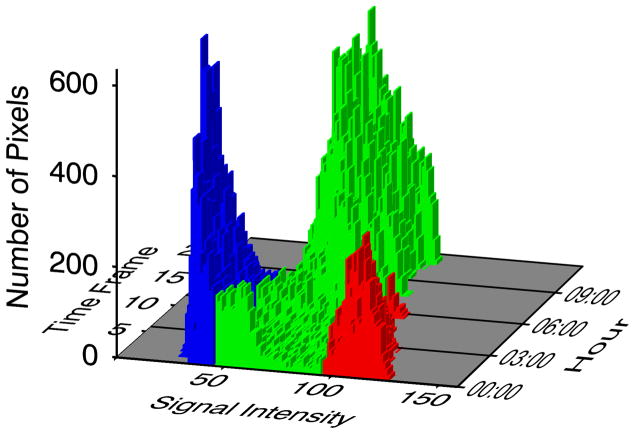
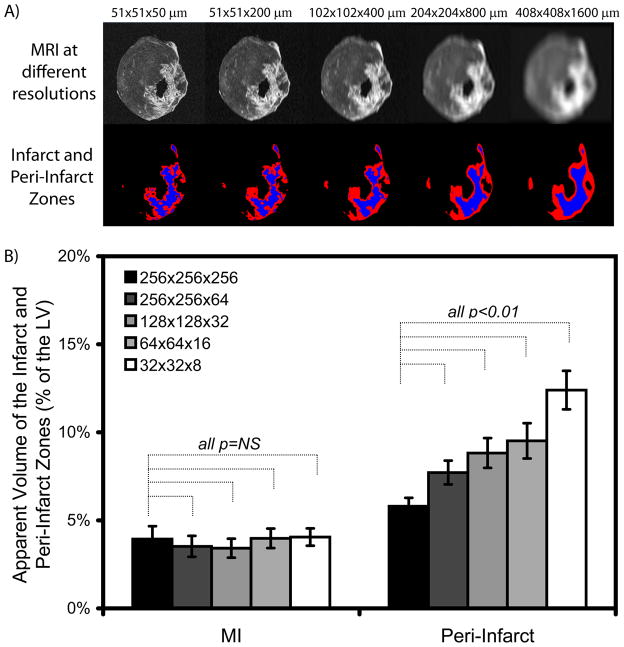
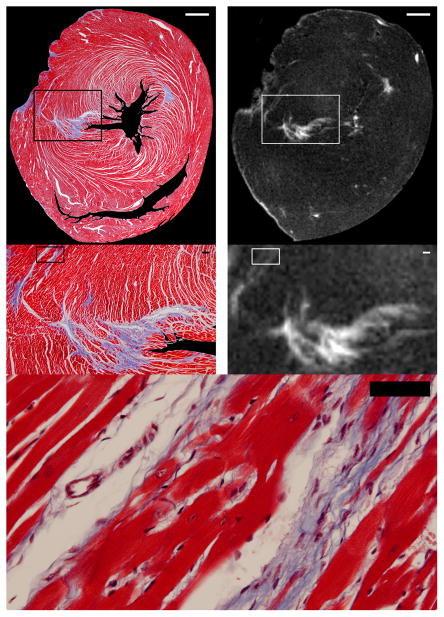
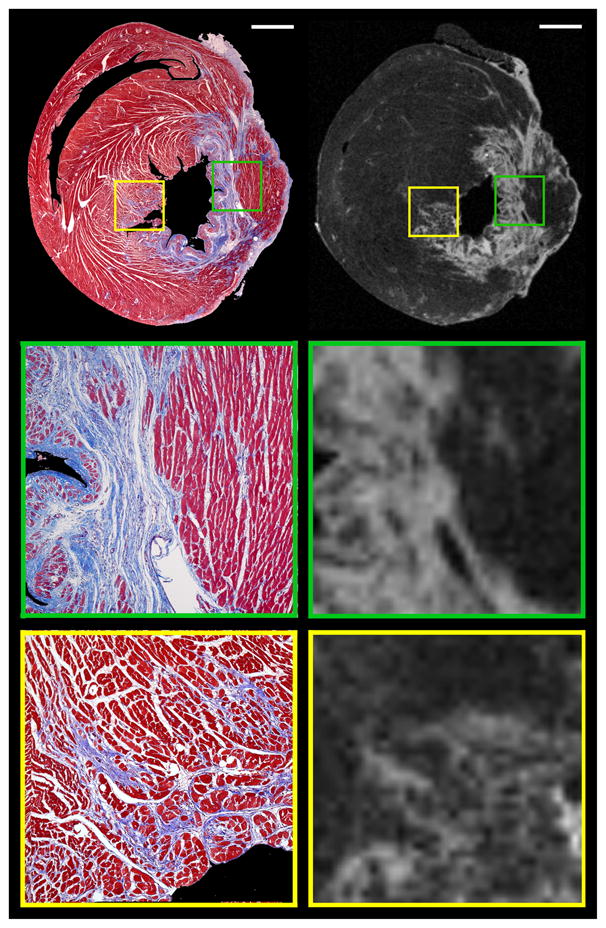
Methods and results: sprague-Dawley rats underwent myocardial infarction by coronary ligation. Two months later, rats were euthanized 10 minutes after administration of 0.3 mmol/kg intravenous gadolinium. LGE images ex vivo at 7 T with a 3D gradient echo sequence with 50×50×50 μm voxels were compared with histological sections (Masson trichrome). Planimetered histological and LGE regions of fibrosis correlated well (y=1.01x-0.01; R(2)=0.96; P<0.001). In addition, LGE images routinely detected clefts of viable cardiomyocytes 2 to 4 cells thick that separated bands of fibrous tissue. Although LGE clearly detected disorganized mixtures of fibrosis and viable cardiomyocytes characterized by intermediate signal intensity voxels, the percentage of apparent intermediate signal intensity myocardium increased significantly (P<0.01) when image resolution was degraded to resemble clinical resolution consistent with significant partial volume averaging.
Conclusions: these data provide important validation of LGE at nearly the cellular level for detection of fibrosis after myocardial infarction. Although LGE can detect heterogeneous patches of fibrosis and viable cardiomyocytes as patches of intermediate signal intensity, the percentage of intermediate signal intensity voxels is resolution dependent. Thus, at clinical resolutions, distinguishing the peri-infarct border zone from partial volume averaging with LGE is challenging.
Figures
References
-
- Karamitsos TD, Francis JM, Myerson S, Selvanayagam JB, Neubauer S. The role of cardiovascular magnetic resonance imaging in heart failure. J Am Coll Cardiol. 2009;54:1407–1424. - PubMed
-
- Choi KM, Kim RJ, Gubernikoff G, Vargas JD, Parker M, Judd RM. Transmural extent of acute myocardial infarction predicts long-term improvement in contractile function. Circulation. 2001;104:1101–1107. - PubMed
-
- Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, Klocke FJ, Bonow RO, Judd RM. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. N Engl J Med. 2000;343:1445–1453. - PubMed
-
- Schvartzman PR, Srichai MB, Grimm RA, Obuchowski NA, Hammer DF, McCarthy PM, Kasper JM, White RD. Nonstress delayed-enhancement magnetic resonance imaging of the myocardium predicts improvement of function after revascularization for chronic ischemic heart disease with left ventricular dysfunction. Am Heart J. 2003;146:535–541. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
