

Transcranial approach to pituitary adenomas invading the cavernous sinus: A modification of the classical technique to be used in a low-technology environment
- PMID: 20847907
- PMCID: PMC2940085
- DOI: 10.4103/2152-7806.65054
Transcranial approach to pituitary adenomas invading the cavernous sinus: A modification of the classical technique to be used in a low-technology environment
Abstract
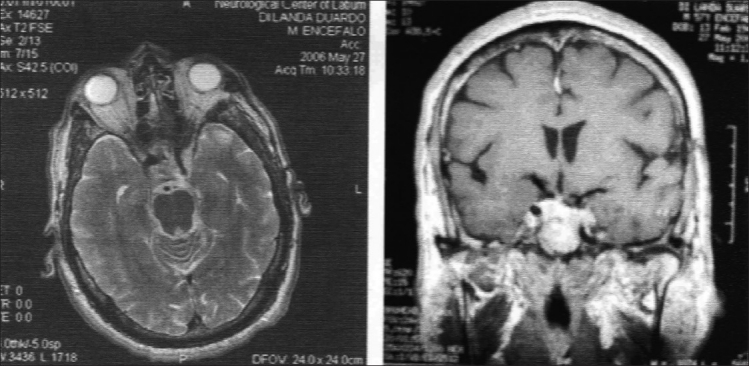
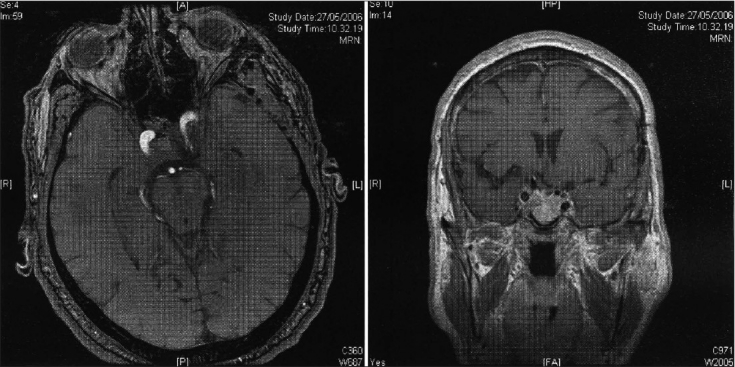
Objective: Pituitary adenomas invading the cavernous sinus represent a therapeutic challenge. Those tumors have been traditionally treated with incomplete surgical removal, observation and/ or adjunctive medical therapy, and radiotherapy. In relatively recent years, some authors have suggested a main direct surgical approach to cavernous sinus (CS) with the aim of complete removal of the adenoma, either by a modified trans-sphenoidal route, using or not an endoscopy-assisted approach, or by a transcranial direct approach. The latter has the advantage of allowing direct exposure of the lesion with a view of the surgical field unhindered by important neurovascular structures.
Materials and methods: We report a technical modification of the classical epidural approach for CS adenoma removal. This was used in 14 patients. Surgical technique included a fronto-orbito-zygomatic craniotomy with extradural anterior clinoidectomy, and intradural approach to the Hakuba's triangle for intracavernous dissection. The tumors were removed under direct vision.
Results: Total macroscopical removal was achieved in all but one case. This patient required postoperative radiation therapy as well as adjuvant dopaminergic regime for achieving control of preoperatively increased hormonal values. No other case required radiotherapy. Hormonal and/ or clinical control was also achieved in all the remaining cases. Out of the remaining 13 cases, all appeared to be tumor free at an average postoperative observation at 78 months (34 to 90 months). Significant surgical sequels were detected in only 1 case (persistent 3(rd) nerve palsy and moderate hemiparesis).
Conclusions: This experience, though limited, would suggest that the transcranial limited CS exposure through the Hakuba's triangle may allow adequate removal of intracavernous pituitary adenomas with very good long-term results and acceptable complication rate.
Keywords: Cavernous sinus surgery; Hakuba’s triangle; fronto-orbito-zygomatic craniotomy (FOZ); invasive adenoma; transcranial approach.
Figures

Similar articles
-
[Pituitary adenomas invading the cavernous sinus. Transcranial transcavernous approach].Neurocirugia (Astur). 2007 Aug;18(4):294-300. doi: 10.4321/s1130-14732007000400002. Neurocirugia (Astur). 2007. PMID: 17882336 Spanish.
-
Hakuba's triangle: a cadaveric study detailing its anatomy and neurovascular contents with vascular and skull base implications.Neurosurg Rev. 2022 Jun;45(3):2087-2093. doi: 10.1007/s10143-021-01707-x. Epub 2022 Jan 7. Neurosurg Rev. 2022. PMID: 34993690
-
Extended transsphenoidal approach for pituitary adenomas invading the anterior cranial base, cavernous sinus, and clivus: a single-center experience with 126 consecutive cases.J Neurosurg. 2010 Jan;112(1):108-17. doi: 10.3171/2009.3.JNS0929. J Neurosurg. 2010. PMID: 19408986
-
The Party Wall: Redefining the Indications of Transcranial Approaches for Giant Pituitary Adenomas in Endoscopic Era.Cancers (Basel). 2023 Apr 10;15(8):2235. doi: 10.3390/cancers15082235. Cancers (Basel). 2023. PMID: 37190164 Free PMC article. Review.
-
Transcranial surgery for pituitary adenomas.Neurosurgery. 2005 Jul;57(1 Suppl):168-75; discussion 168-75. doi: 10.1227/01.neu.0000163602.05663.86. Neurosurgery. 2005. PMID: 15987585 Review.
Cited by
-
Endoscopic transnasal suprasellar approach for anterior clinoidal meningioma: A case report and review of the literature.Surg Neurol Int. 2017 Aug 22;8:194. doi: 10.4103/sni.sni_147_17. eCollection 2017. Surg Neurol Int. 2017. PMID: 28904821 Free PMC article.
-
Outcomes and Complications of Aggressive Resection Strategy for Pituitary Adenomas in Knosp Grade 4 With Transsphenoidal Endoscopy.Front Oncol. 2021 Jun 21;11:693063. doi: 10.3389/fonc.2021.693063. eCollection 2021. Front Oncol. 2021. PMID: 34235083 Free PMC article.
-
Cavernous Sinus Involvement by Pituitary Adenomas: Clinical Implications and Outcomes of Endoscopic Endonasal Resection.J Neurol Surg B Skull Base. 2017 Jun;78(3):273-282. doi: 10.1055/s-0036-1598022. Epub 2017 Jan 23. J Neurol Surg B Skull Base. 2017. PMID: 28603683 Free PMC article.
-
Endoscopic endonasal trans-sphenoid surgery of pituitary adenoma.J Neurosci Rural Pract. 2012 Sep;3(3):328-37. doi: 10.4103/0976-3147.102615. J Neurosci Rural Pract. 2012. PMID: 23188987 Free PMC article.
References
-
- Ahmadi J, North CM, Segall HD, Zee CS, Weiss MH. Cavernous sinus invasion by pituitary adenomas. AJR Am J Roentgenol. 1986;146:257–62. - PubMed
-
- Al-Mefty O, Smith RR. Surgery of tumours invading the cavernous sinus. Surg Neurol. 1988;30:370–81. - PubMed
-
- Cappabianca P, Alfieri A, de Divitiis E. Endoscopic endonasal transsphenoidal approach to the sella: Towards functional endoscopic pituitary surgery (FEPS) Minim Invasive Neurosurg. 1998;41:66–73. - PubMed
-
- Cavallo LM, Cappabianca P, Galzio R, Iaconetta G, de Divitiis E, Tschabitscher M. Endoscopic transnasal approach to the cavernous sinus versus transcranial route: Anatomic study. Neurosurgery. 2005;56:379–88. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
