

Percutaneous vertebroplasty relieves pain in metastatic cervical fractures
- PMID: 20848245
- PMCID: PMC3032872
- DOI: 10.1007/s11999-010-1550-y
Percutaneous vertebroplasty relieves pain in metastatic cervical fractures
Abstract
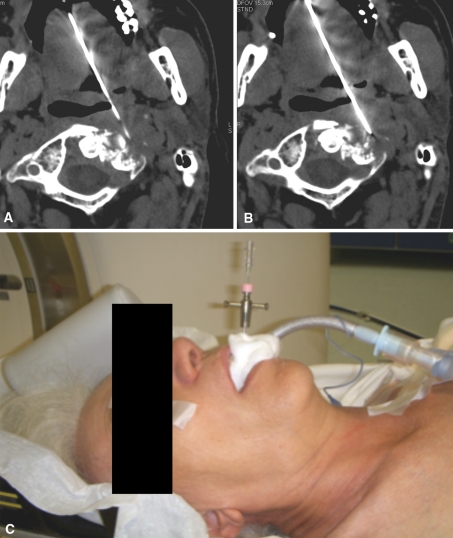
Background: Percutaneous vertebroplasty is currently an alternative for treating vertebral fractures of the thoracic and lumbar spine, providing both pain control and vertebral stabilization. In the cervical spine, however, percutaneous vertebroplasty is technically challenging because of the complex anatomy of this region.
Questions/purposes: We evaluated the technical feasibility, complication rate, and ability of percutaneous vertebroplasty to provide pain relief in patients with painful metastatic cervical fractures.
Methods: We retrospectively reviewed 62 patients (24 men) who, between May 2005 and May 2009, underwent vertebroplasty to treat painful metastatic cervical fractures. Each patient was evaluated by a visual analog scale for pain, number of pain analgesics, and CT and MRI before, the day after, and at 3 months after the procedure.
Results: Two of the 62 patients had asymptomatic cement leakage in the soft tissues. We observed no delayed complications. Mean pretreatment and 24-hour posttreatment visual analog scale pain scores were 7.9±1.7 and 1.5±2, respectively. Immediately after surgery, the pain completely disappeared in 25 (40%) patients. Administration of analgesics was suspended in 34 (55%) patients whereas in 27 (39%) patients the median analgesics use decreased from two pills per day (range, 0-3) to 0 (range, 0-3). In two (3%) patients, analgesics administration was continued due to the persistence of pain. At 3 months, the patients reported a mean visual analog scale pain score of 1.7±2.
Conclusions: Our data suggest, in selected patients, percutaneous vertebroplasty may be performed with a high technical success rate combined with a low complication rate, providing immediate pain relief lasting at least 3 months and a reduction in the use of analgesic drugs.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures

References
-
- Barr JD, Barr MS, Lemley TJ, McCann RM. Percutaneous vertebroplasty for pain relief and spinal stabilization. Spine (Phila Pa 1976) 2000;25:923–928. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
