

Synovial tissue-infiltrating natural killer cells in osteoarthritis and periprosthetic inflammation
- PMID: 20848566
- PMCID: PMC2995813
- DOI: 10.1002/art.27751
Synovial tissue-infiltrating natural killer cells in osteoarthritis and periprosthetic inflammation
Abstract
Objective: Infiltrating immune cells play a central role in degenerative joint disease associated with osteoarthritis (OA) and particle-mediated periprosthetic osteolysis. The goal of this study was to characterize a newly identified population of synovial tissue-infiltrating natural killer (NK) cells obtained from patients with OA or patients with periprosthetic joint inflammation.
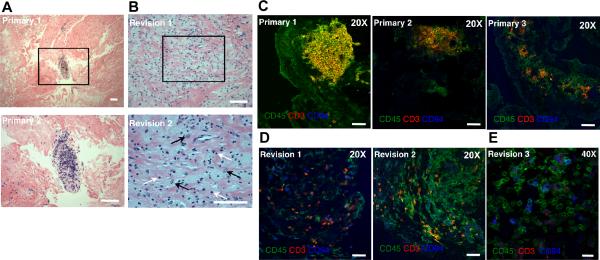
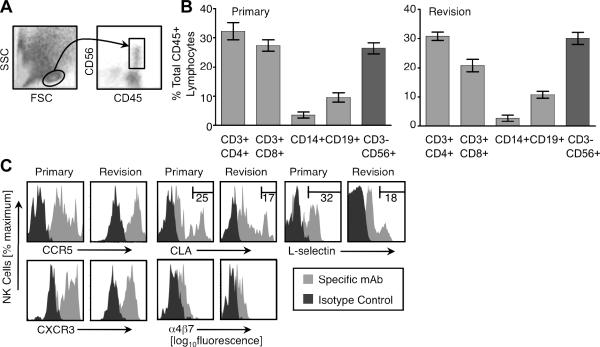
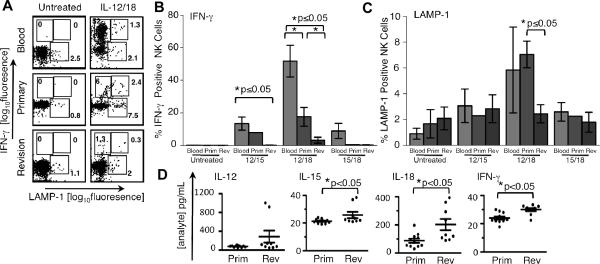
Methods: Synovial and interfacial tissue samples were collected from patients with OA who were undergoing primary or revision total joint replacement (TJR) surgery. The histologic features of OA synovium obtained from patients undergoing primary surgery and interfacial tissue obtained from patients undergoing revision surgery were determined by immunohistochemistry and immunofluorescence. Synovial tissue-infiltrating NK cells were evaluated for the expression of surface receptors, using flow cytometry. Chemoattractant and cytokine protein and RNA levels in synovial and interfacial tissue and fluid were assessed by Luminex assay and real-time quantitative polymerase chain reaction. Cytokine production and degranulation by stimulated synovial tissue versus normal blood NK cells were evaluated by intracellular cytokine staining.
Results: NK cells comprised nearly 30% of the CD45+ mononuclear cell infiltrate in synovial tissue obtained from patients undergoing primary TJR and from patients undergoing revision TJR. NK cells from both groups expressed CXCR3, CCR5, L-selectin, α4 integrins, and cutaneous lymphocyte antigen. Synovial fluid from patients undergoing revision surgery contained elevated concentrations of the NK cell attractants CCL4, CCL5, CXCL9, and CXCL10; all levels in synovial fluid obtained from patients undergoing revision surgery were higher than those in synovial fluid from patients undergoing primary surgery. Cytokine-stimulated interferon-γ production was significantly impaired in NK cells derived from primary and revision TJRs compared with blood NK cells.
Conclusion: NK cells are a principal tissue-infiltrating lymphocyte subset in patients with OA and patients with periprosthetic inflammation and display a quiescent phenotype that is consistent with postactivation exhaustion.
Copyright © 2010 by the American College of Rheumatology.
Figures
References
-
- Schulte KR, Callaghan JJ, Kelley SS, Johnston RC. The outcome of Charnley total hip arthroplasty with cement after a minimum twenty-year follow-up. The results of one surgeon. J Bone Joint Surg Am. 1993;75(7):961–75. - PubMed
-
- Callaghan JJ, Bracha P, Liu SS, Piyaworakhun S, Goetz DD, Johnston RC. Survivorship of a Charnley total hip arthroplasty. A concise follow-up, at a minimum of thirty-five years, of previous reports. J Bone Joint Surg Am. 2009;91(11):2617–21. - PubMed
-
- Huddleston JI, Maloney WJ, Wang Y, Verzier N, Hunt DR, Herndon JH. Adverse events after total knee arthroplasty: a national Medicare study. J Arthroplasty. 2009;24(6 Suppl):95–100. - PubMed
-
- Ottaviani C, Nasorri F, Bedini C, de Pita O, Girolomoni G, Cavani A. CD56brightCD16(−) NK cells accumulate in psoriatic skin in response to CXCL10 and CCL5 and exacerbate skin inflammation. Eur J Immunol. 2006;36(1):118–28. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R37 GM037734/GM/NIGMS NIH HHS/United States
- R37 AI047822/AI/NIAID NIH HHS/United States
- R01-AR-55650/AR/NIAMS NIH HHS/United States
- HL-67674/HL/NHLBI NIH HHS/United States
- AI-47822/AI/NIAID NIH HHS/United States
- R21 AI059635/AI/NIAID NIH HHS/United States
- R01 AI059635/AI/NIAID NIH HHS/United States
- P50 HL067674/HL/NHLBI NIH HHS/United States
- P30 DK056339/DK/NIDDK NIH HHS/United States
- P01 HL067674/HL/NHLBI NIH HHS/United States
- R01 AI047822/AI/NIAID NIH HHS/United States
- HHMI/Howard Hughes Medical Institute/United States
- AI-59635/AI/NIAID NIH HHS/United States
- GM-37734/GM/NIGMS NIH HHS/United States
- R01 AI079320/AI/NIAID NIH HHS/United States
- DK-56339/DK/NIDDK NIH HHS/United States
- R01 GM037734/GM/NIGMS NIH HHS/United States
- R01 AR055650/AR/NIAMS NIH HHS/United States
- AI-079320/AI/NIAID NIH HHS/United States
- R21 AI047822/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
