

An educational approach based on a non-injury model compared with individual symptom-based physical training in chronic LBP. A pragmatic, randomised trial with a one-year follow-up
- PMID: 20849601
- PMCID: PMC2954985
- DOI: 10.1186/1471-2474-11-212
An educational approach based on a non-injury model compared with individual symptom-based physical training in chronic LBP. A pragmatic, randomised trial with a one-year follow-up
Abstract
Background: In the treatment of chronic back pain, cognitive methods are attracting increased attention due to evidence of effectiveness similar to that of traditional therapies. The purpose of this study was to compare the effectiveness of performing a cognitive intervention based on a non-injury model with that of a symptom-based physical training method on the outcomes of low back pain (LBP), activity limitation, LBP attitudes (fear-avoidance beliefs and back beliefs), physical activity levels, sick leave, and quality of life, in chronic LBP patients.
Methods: The study was a pragmatic, single-blind, randomised, parallel-group trial. Patients with chronic/recurrent LBP were randomised to one of the following treatments: 1. Educational programme : the emphasis was on creating confidence that the back is strong, that loads normally do not cause any damage despite occasional temporary pain, that reducing the focus on the pain might facilitate more natural and less painful movements, and that it is beneficial to stay physically active. 2. Individual symptom-based physical training programme : directional-preference exercises for those centralising their pain with repetitive movements; 'stabilising exercises' for those deemed 'unstable' based on specific tests; or intensive dynamic exercises for the remaining patients. Follow-up questionnaires (examiner-blinded) were completed at 2, 6 and 12 months. The main statistical test was an ANCOVA adjusted for baseline values.
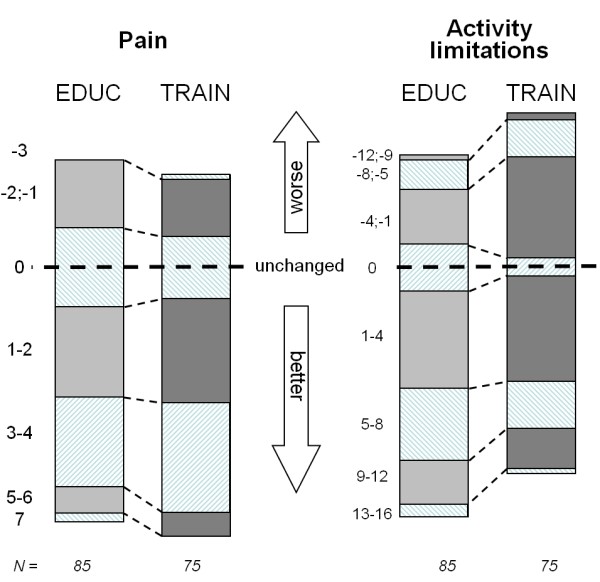
Results: A total of 207 patients participated with the median age of 39 years (IQR 33-47); 52% were female, 105 were randomised to the educational programme and 102 to the physical training programme. The two groups were comparable at baseline. For the primary outcome measures, there was a non-significant trend towards activity limitation being reduced mostly in the educational programme group, although of doubtful clinical relevance. Regarding secondary outcomes, improvement in fear-avoidance beliefs was also better in the educational programme group. All other variables were about equally influenced by the two treatments. The median number of treatment sessions was 3 for the educational programme group and 6 for the physical training programme group.
Conclusions: An educational approach to treatment for chronic LBP resulted in at least as good outcomes as a symptom-based physical training method, despite fewer treatment sessions.
Trial registration: ClinicalTrials.gov NCT00410319.
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
