

Performance of small general practices under the UK's Quality and Outcomes Framework
- PMID: 20849683
- PMCID: PMC2930243
- DOI: 10.3399/bjgp10X515340
Performance of small general practices under the UK's Quality and Outcomes Framework
Abstract
Background: Small general practices are often perceived to provide worse care than larger practices.
Aim: To describe the comparative performance of small practices on the UK's pay-for-performance scheme, the Quality and Outcomes Framework.
Design of study: Longitudinal analysis (2004-2005 to 2006-2007) of quality scores for 48 clinical activities.
Setting: Family practices in England (n = 7502).
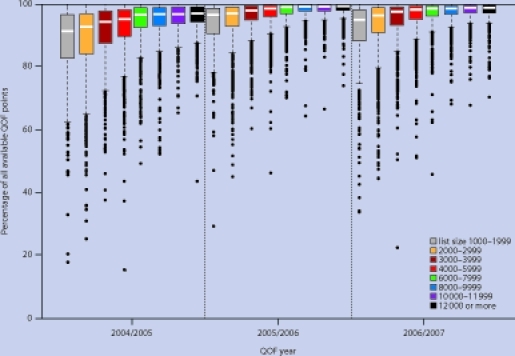
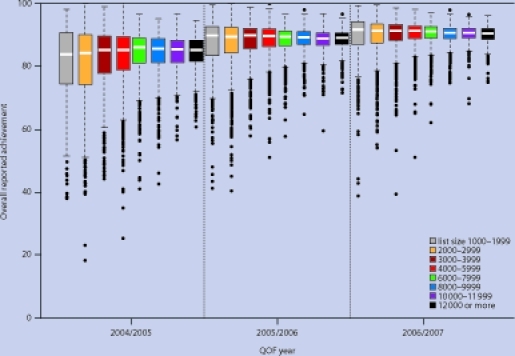
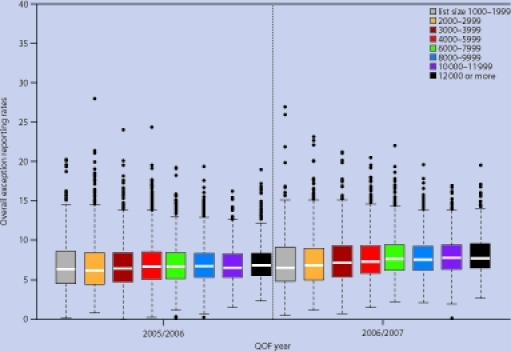
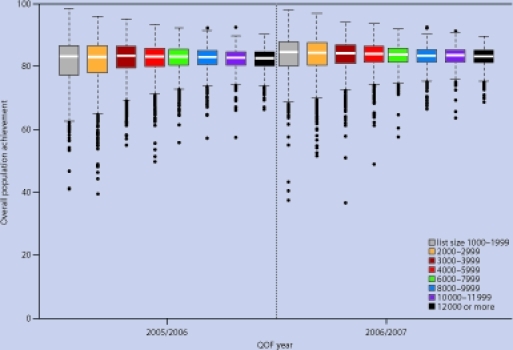
Method: Comparison of performance of practices by list size, in terms of points scored in the pay-for-performance scheme, reported achievement rates, and population achievement rates (which allow for patients excluded from the scheme).
Results: In the first year of the pay-for-performance scheme, the smallest practices (those with fewer than 2000 patients) had the lowest median reported achievement rates, achieving the clinical targets for 83.8% of eligible patients. Performance generally improved for practices of all sizes over time, but the smallest practices improved at the fastest rate, and by year 3 had the highest median reported achievement rates (91.5%). This improvement was not achieved by additional exception reporting. There was more variation in performance among small practices than larger ones: practices with fewer than 3000 patients (20.1% of all practices in year 3), represented 46.7% of the highest-achieving 5% of practices and 45.1% of the lowest-achieving 5% of practices.
Conclusion: Small practices were represented among both the best and the worst practices in terms of achievement of clinical quality targets. The effect of the pay-for-performance scheme appears to have been to reduce variation in performance, and to reduce the difference between large and small practices.
Figures
References
-
- Secretary of State for Health. The NHS Plan: a plan for investment. A plan for reform. London: The Stationery Office; 2000. Cm 4818–1.
-
- Smith J. Safeguarding patients: lessons from the past — proposals for the future. London: HMSO; 2004. Shipman Inquiry Fifth Report. Cm 6394.
-
- Audit Commission. A focus on general practice in England. London: Audit Commission; 2002.
-
- Department of Health. High quality care for all: NHS next stage review. London: Department of Health; 2008.
-
- Roland M. Linking physicians’ pay to the quality of care — a major experiment in the United Kingdom. N Engl J Med. 2004;351(14):1448–1454. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources