

Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database
- PMID: 20853057
- PMCID: PMC4324560
- DOI: 10.1245/s10434-010-1253-3
Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database
Abstract
Background: Complete axillary lymph node dissection (ALND) after a positive sentinel lymph node biopsy (SLNB) remains the standard practice. As nodal surgery has long been considered a staging procedure without a clear survival benefit, the need for ALND in all patients is debatable. The purpose of this study was to examine differences in survival for patients undergoing SLNB alone versus SLNB with complete ALND.
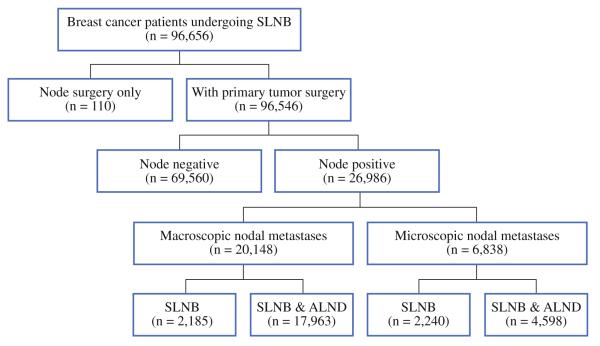
Methods: Patients with breast cancer who underwent SLNB and were found to have nodal metastases were identified from the Surveillance, Epidemiology, and End Results database (1998-2004). Clinicopathologic and outcomes data were examined for patients who underwent SLNB alone versus SLNB with ALND.
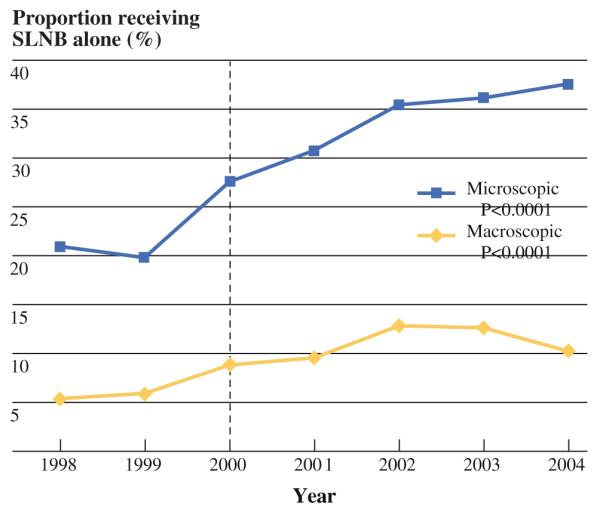
Results: We identified 26,986 patients with disease-positive lymph nodes; 4,425 (16.4%) underwent SLNB alone, and 22,561 (83.6%) underwent SLNB with ALND. Patients were significantly more likely to undergo SLNB alone if they were older (median 59 years old) or if the tumor was low grade and estrogen receptor positive. From 1998 to 2004, the proportion of patients with micrometastasis in the sentinel lymph nodes who underwent SLNB alone increased from 21.0 to 37.8% (P < 0.001). At a median follow-up of 50 months, there were no statistically significant differences in overall survival (OS) between patients who underwent SLNB alone versus complete ALND.
Conclusions: There is an increasing trend toward omitting ALND in patients with micrometastatic nodal disease identified by SLNB. Compared with SLNB alone, completion ALND does not seem to be associated with improved survival for breast cancer patients with micrometastasis in the sentinel lymph nodes.
Figures
Comment in
-
Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: a practice-changing trial.Ann Surg Oncol. 2011 Sep;18(9):2407-12. doi: 10.1245/s10434-011-1593-7. Ann Surg Oncol. 2011. PMID: 21327455 Free PMC article. No abstract available.
References
-
- Benson K, Hartz AJ. A comparison of observational studies and randomized, controlled trials. Am J Ophthalmol. 2000;130:688. - PubMed
-
- Lyman GH, Giuliano AE, Somerfield MR, et al. American Society of Clinical Oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol. 2005;23:7703–20. - PubMed
-
- National Comprehensive Cancer Network (NCCN) clinical practice guidelines in oncology: breast [Accessed on 1 Mar 2010];2008 http://www.nccn.org/professionals/physiciangls/PDF/breast.pdf.
-
- Guenther JM, Hansen NM, DiFronzo LA, et al. Axillary dissection is not required for all patients with breast cancer and positive sentinel nodes. Arch Surg. 2003;138:52–6. - PubMed
-
- Jeruss JS, Winchester DJ, Sener SF, et al. Axillary recurrence after sentinel node biopsy. Ann Surg Oncol. 2005;12:34–40. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
