

National trends in child and adolescent psychotropic polypharmacy in office-based practice, 1996-2007
- PMID: 20855045
- PMCID: PMC2952543
- DOI: 10.1016/j.jaac.2010.07.007
National trends in child and adolescent psychotropic polypharmacy in office-based practice, 1996-2007
Abstract
Objective: To examine patterns and recent trends in multiclass psychotropic treatment among youth visits to office-based physicians in the United States.
Method: Annual data from the 1996-2007 National Ambulatory Medical Care Surveys were analyzed to examine patterns and trends in multiclass psychotropic treatment within a nationally representative sample of 3,466 child and adolescent visits to office-based physicians in which a psychotropic medication was prescribed.
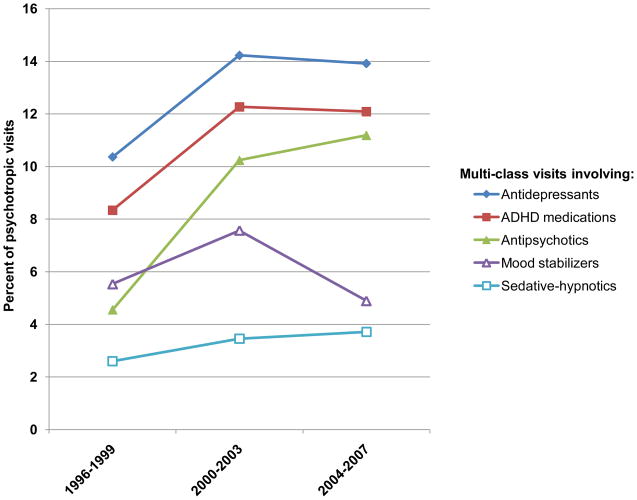
Results: There was an increase in the percentage of child visits in which psychotropic medications were prescribed that included at least two psychotropic classes. Across the 12 year period, multiclass psychotropic treatment rose from 14.3% of child psychotropic visits (1996-1999) to 20.2% (2004-2007) (adjusted odds ratio [AOR] = 1.89, 95% confidence interval [CI] = 1.22-2.94, p < .01). Among medical visits in which a current mental disorder was diagnosed, the percentage with multiclass psychotropic treatment increased from 22.2% (1996-1999) to 32.2% (2004-2007) (AOR = 2.23, 95% CI = 1.42-3.52, p < .001). Over time, there were significant increases in multiclass psychotropic visits in which ADHD medications, antidepressants, or antipsychotics were prescribed, and a decrease in those visits in which mood stabilizers were prescribed. There were also specific increases in co-prescription of ADHD medications and antipsychotic medications (AOR = 6.22, 95% CI = 2.82-13.70, p < .001) and co-prescription of antidepressant and antipsychotic medications (AOR = 5.77, 95% CI = 2.88-11.60, p < .001).
Conclusions: Although little is known about the safety and efficacy of regimens that involve concomitant use of two or more psychotropic agents for children and adolescents, multiclass psychotropic pharmacy is becoming increasingly common in outpatient practice.
Copyright © 2010 American Academy of Child and Adolescent Psychiatry. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- AACAP Work Group on Quality Issues. Practice parameter on the use of psychotropic medication in children and adolescents. J Am Acad Child Adolesc Psychiatry. 2009;48:961–973. - PubMed
-
- Swanson JM, Kraemer HC, Hinshaw SP, et al. Clinical relevance of the primary findings of the MTA: Success rates based on severity of ADHD and ODD symptoms at the end of treatment. J Am Acad Child Adolesc Psychiatry. 2002;40:168–179. - PubMed
-
- Bridge JA, Iyengar S, Salary CB, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials. JAMA. 2007;297:1683–1696. - PubMed
-
- TADS Team. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescetns with Depression Study (TADS) randomized controlled trial. JAMA. 2004;292:807–820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
