

Noninvasive characterization of epicardial activation in humans with diverse atrial fibrillation patterns
- PMID: 20855661
- PMCID: PMC2996091
- DOI: 10.1161/CIRCULATIONAHA.110.945709
Noninvasive characterization of epicardial activation in humans with diverse atrial fibrillation patterns
Abstract
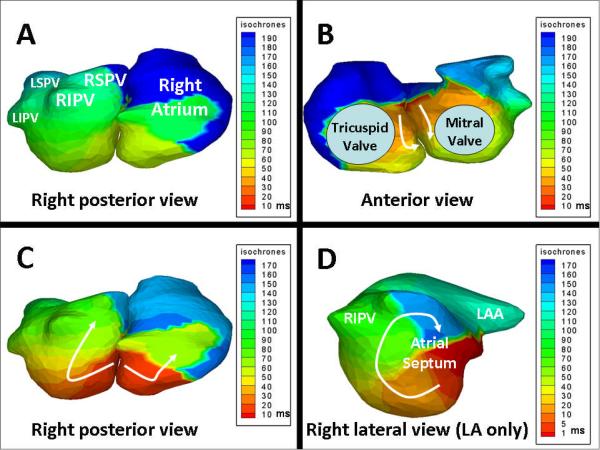
Background: Various mechanisms of atrial fibrillation (AF) have been demonstrated experimentally. Invasive methods to study these mechanisms in humans have limitations, precluding continuous mapping of both atria with sufficient resolution. In this article, we present continuous biatrial epicardial activation sequences of AF in humans using noninvasive electrocardiographic imaging (ECGI).
Methods and results: In the testing phase, ECGI accuracy was evaluated by comparing ECGI with co-registered CARTO images during atrial pacing in 6 patients. Additionally, correlative observations from catheter mapping and ablation were compared with ECGI in 3 patients. In the study phase, ECGI maps during AF in 26 patients were analyzed for mechanisms and complexity. ECGI noninvasively imaged the low-amplitude signals of AF in a wide range of patients (97 procedural success). Spatial accuracy for determining initiation sites from pacing was 6 mm. Locations critical to maintenance of AF identified during catheter ablation were identified by ECGI; ablation near these sites restored sinus rhythm. In the study phase, the most common patterns of AF were multiple wavelets (92), with pulmonary vein (69) and non-pulmonary vein (62) focal sites. Rotor activity was seen rarely (15). AF complexity increased with longer clinical history of AF, although the degree of complexity of nonparoxysmal AF varied widely.
Conclusions: ECGI offers a noninvasive way to map epicardial activation patterns of AF in a patient-specific manner. The results highlight the coexistence of a variety of mechanisms and variable complexity among patients. Overall, complexity generally increased with duration of AF.
Figures







References
-
- Stewart S, Hart CL, Hole DJ, McMurray JJ. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am J Med. 2002;113:359–64. - PubMed
-
- Wattigney WA, Mensah GA, Croft JB. Increasing trends in hospitalization for atrial fibrillation in the United States, 1985 through 1999. Circulation. 2003;108:711–6. - PubMed
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC, Jr., Jacobs AK, Adams CD, Anderson JL, Antman EM, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Zamorano JL. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation. Circulation. 2006;114:e257–354. - PubMed
-
- Jalife J, Berenfeld O, Mansour M. Mother rotors and fibrillatory conduction: a mechanism of atrial fibrillation. Cardiovasc Res. 2002;54:204–16. - PubMed
-
- Chen YJ, Chen SA. Electrophysiology of pulmonary veins. J Cardiovasc Electrophysiol. 2006;17:220–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
