

Safety and efficacy of moxifloxacin monotherapy for treatment of orthopedic implant-related staphylococcal infections
- PMID: 20855727
- PMCID: PMC2981285
- DOI: 10.1128/AAC.00027-10
Safety and efficacy of moxifloxacin monotherapy for treatment of orthopedic implant-related staphylococcal infections
Abstract
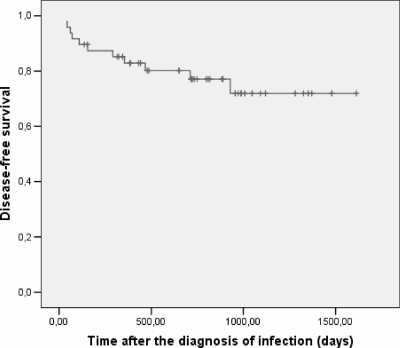
The rifampin-ciprofloxacin combination is recommended for treatment of orthopedic implant-related staphylococcal infections to avoid the emergence of ciprofloxacin resistance; however, the efficacy of this combination is limited by the tolerability problems associated with the use of rifampin. Moxifloxacin is a quinolone up to 10 times more active against staphylococci than ciprofloxacin and the risk of resistance development during monotherapy against staphylococci is theoretically lower for moxifloxacin, but information regarding its use in bone infections is lacking. The aim of the present study was to evaluate the safety and clinical efficacy of moxifloxacin monotherapy in patients with orthopedic implant-related staphylococcal infections. From June 2006 to April 2009, all patients with culture-proven infection by quinolone-sensitive staphylococcal strains associated with orthopedic implants at our institution were included in a management protocol that mostly included specific surgery, 1 to 2 weeks of an intravenous course of cloxacillin-cefazolin or vancomycin, and long-term therapy with moxifloxacin (400 mg/day for 3 months). Cure was defined as (i) a lack of clinical signs and symptoms of infection, (ii) a C-reactive protein level less than 5 mg/liter, and (iii) absence of radiological signs of loosening or infection at the latest follow-up visit. Failure was defined as (i) persisting clinical and/or laboratory signs of infection or (ii) persisting or new isolation of the initial microorganism. A total of 48 patients with a median follow-up of 716 days (range, 102 to 1,613 days) were included in the study. Complete drug compliance was achieved in all but two patients (4.2%), who required drug discontinuation because of side effects (diarrhea and dizziness). No moxifloxacin-induced arrhythmia was reported. Twenty patients had joint prosthesis infections (5 acute-onset infections and 15 chronic infections), and 28 patients had osteosynthesis material infections (4 acute-onset infections and 24 chronic infections). The etiologies were methicillin-sensitive Staphylococcus aureus in 33 patients and a coagulase-negative staphylococcus (CoNS) in 15. Surgical management was performed for the majority of patients (37/48; 77%), and the implant was retained in 21 patients (43.8%). The global cure rate was 38/46 (82.6%), and the cure rate for patients with implant retention was 15/21 (71.4%). The global cure rate for the 32 patients with a minimum follow-up of 2 years was 80%. Of the eight cases of relapse, we obtained microbiological confirmation in six cases, and all bacteria recovered were quinolone susceptible. Monotherapy with moxifloxacin seems to be an effective, safe, and easy alternative for the long-term treatment of orthopedic implant-related staphylococcal infections by quinolone-sensitive strains. Comparative studies with rifampin-containing regimens are warranted.
Figures


References
-
- Bahl, D., D. A. Miller, I. Leviton, P. Gialanella, M. J. Wolin, W. Liu, R. Perkins, and M. H. Miller. 1997. In vitro activities of ciprofloxacin and rifampin alone and in combination against growing and nongrowing strains of methicillin-susceptible and methicillin-resistant Staphylococcus aureus. Antimicrob. Agents Chemother. 41:1293-1297. - PMC - PubMed
-
- Barberan, J., L. Aguilar, G. Carroquino, M. J. Gimenez, B. Sanchez, D. Martinez, and J. Prieto. 2006. Conservative treatment of staphylococcal prosthetic joint infections in elderly patients. Am. J. Med. 119:993.e7-e10. - PubMed
-
- Barberan, J., L. Aguilar, M. J. Gimenez, G. Carroquino, J. J. Granizo, and J. Prieto. 2008. Levofloxacin plus rifampicin conservative treatment of 25 early staphylococcal infections of osteosynthetic devices for rigid internal fixation. Int. J. Antimicrob. Agents 32:154-157. - PubMed
-
- Brandt, C. M., M. C. Duffy, E. F. Berbari, A. D. Hanssen, J. M. Steckelberg, and D. R. Osmon. 1999. Staphylococcus aureus prosthetic joint infection treated with prosthesis removal and delayed reimplantation arthroplasty. Mayo Clin. Proc. 74:553-558. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
