

Sex-based outcomes of darunavir-ritonavir therapy: a single-group trial
- PMID: 20855799
- PMCID: PMC3056066
- DOI: 10.7326/0003-4819-153-6-201009210-00002
Sex-based outcomes of darunavir-ritonavir therapy: a single-group trial
Abstract
Background: Women account for an increasing proportion of patients with HIV-1 but remain underrepresented in antiretroviral clinical trials.
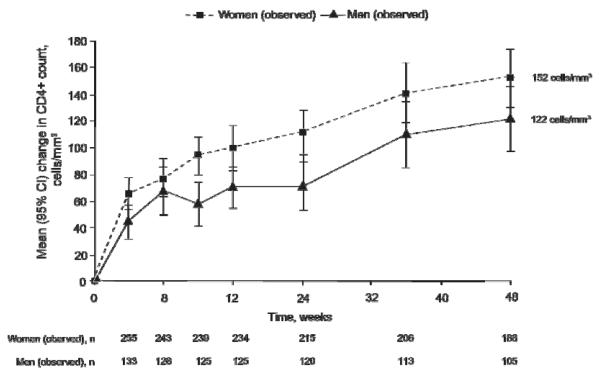
Objective: To evaluate sex-based differences in efficacy and adverse events in treatment-experienced, HIV-positive women and men receiving darunavir-ritonavir therapy over 48 weeks.
Design: Multicenter, open-label, phase 3b study designed to enroll a high proportion of women, with sample size determined on the basis of a noninferiority design with a maximum allowable difference of 15% in virologic response favoring men. (ClinicalTrials.gov registration number: NCT00381303)
Setting: 65 sites in the United States, Puerto Rico, and Canada.
Patients: 287 women and 142 men.
Intervention: Patients received darunavir-ritonavir, 600/100 mg twice daily, plus an investigator-selected optimized background regimen.
Measurements: Virologic response (HIV RNA <50 copies/mL using a time-to-loss of virologic response [TLOVR] algorithm) and adverse events were assessed over 48 weeks.
Results: 67% of patients were women; 84% of patients were black or Hispanic. A higher proportion of women discontinued treatment than men (32.8% vs. 23.2%; P = 0.042); more women than men discontinued treatment for reasons other than virologic failure. Response rates in women and men at week 48 were 50.9% and 58.5%, respectively (intention-to-treat TLOVR), and 73.0% and 73.5%, respectively (TLOVR censored for patients who withdrew for reasons other than virologic failure). The absolute difference in response, based on logistic regression and adjusted for baseline log(10) viral load and CD4(+) cell count, was -9.6 percentage points (95% CI, -19.9 to 0.7 percentage points; P = 0.067) for intention-to-treat TLOVR and -3.9 percentage points (CI, -13.9 to 6.0 percentage points; P = 0.438) for TLOVR population that censored patients who withdrew for reasons other than virologic failure. Adverse events were similar between the sexes. The most common grade 2 to 4 adverse events that were considered at least possibly treatment related in women and men were nausea (5.2% and 2.8%, respectively), diarrhea (4.5% and 4.9%, respectively), and rash (2.1% and 2.8%, respectively).
Limitation: Baseline characteristics differed between sexes.
Conclusion: Nonsignificant, sex-based differences in response were found during the 48-week study; however, these differences were probably due to higher discontinuation rates in women, suggesting that additional efforts are needed to retain women in clinical trials.
Figures


References
-
- Centers for Disease Control and Prevention (CDC) HIV prevalence estimates---United States, 2006. MMWR Morb Mortal Wkly Rep. 2008;57:1073–6. [PMID: 18830210] - PubMed
-
- Centers for Disease Control and Prevention HIV/AIDS surveillance report. Cases of HIV infection and AIDS in the United States and Dependent Areas. [26 July 2010]. 2007. Accessed at www.cdc.gov/hiv/topics/surveillance/resources/reports/2007report/pdf/200... on.
-
- Centers for Disease Control and Prevention HIV/AIDS among women. [26 July 2010]. Accessed at www.cdc.gov/hiv/topics/women/resources/factsheets/pdf/women.pdf on.
-
- US Census Bureau US fact sheet. 2005–2007 American community survey 3-year estimates. [26 July 2010]. Accessed at http://factfinder.census.gov/servlet/ACSSAFFFacts?_event=&geo_id=01000US....
-
- Zorrilla C, Agrait V. Why do we need the GRACE (Gender, Race, And Clinical Experience) study? Futur HIV Ther. 2007;1:357–63.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials