

Quantification of diffuse myocardial fibrosis and its association with myocardial dysfunction in congenital heart disease
- PMID: 20855860
- PMCID: PMC3048790
- DOI: 10.1161/CIRCIMAGING.108.842096
Quantification of diffuse myocardial fibrosis and its association with myocardial dysfunction in congenital heart disease
Abstract
Background: the etiology of ventricular dysfunction in adult congenital heart disease (ACHD) is not well understood. Diffuse fibrosis is a likely common final pathway and is quantifiable using MRI.
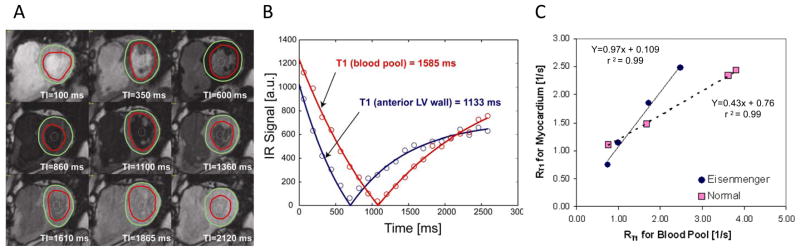
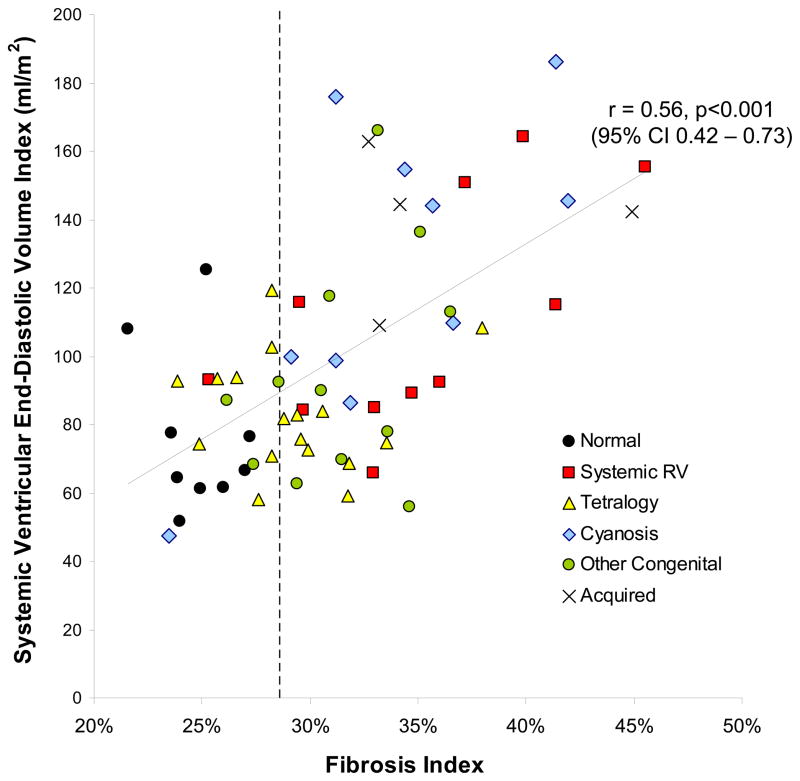
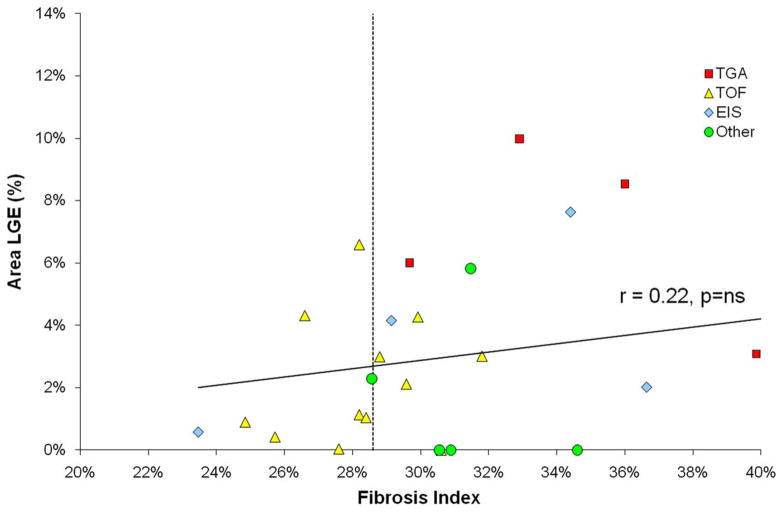
Methods and results: patients with ACHD (n=50) were studied with cardiac MRI to quantify systemic ventricular volume and function and diffuse fibrosis. The fibrosis index for a single midventricular plane of the systemic ventricle was quantified by measuring T1 values for blood pool and myocardium before and after administration of gadolinium (0.15 mmol/kg) and then adjusted for hematocrit. Results were compared to healthy volunteers (normal controls, n=14) and patients with acquired heart failure (positive controls, n=4). Patients studied (age, 37±12 years; female sex, 40%) included 11 with a systemic right ventricle (RV), 17 with tetralogy of Fallot, 10 with cyanosis, and 12 with other lesions. The fibrosis index was significantly elevated in patients with ACHD compared to normal controls (31.9±4.9% versus 24.8±2.0%; P=0.001). Values were highest in patients with a systemic RV (35.0±5.8%; P<0.001) and those who were cyanotic (33.7±5.6%; P<0.001). The fibrosis index correlated with end-diastolic volume index (r=0.60; P<0.001) and ventricular ejection fraction (r=-0.53; P<0.001) but not with age or oxygen saturation in patients who were cyanotic. Late gadolinium enhancement did not account for the differences seen.
Conclusions: patients with ACHD have evidence of diffuse, extracellular matrix remodeling similar to patients with acquired heart failure. The fibrosis index may facilitate studies on the mechanisms and treatment of myocardial fibrosis and heart failure in these patients.
Figures

References
-
- Bolger AP, Coats AJ, Gatzoulis MA. Congenital heart disease: the original heart failure syndrome. Eur Heart J. 2003;24:970–976. - PubMed
-
- Marelli AJ, Mackie AS, Ionescu-Ittu R, Rahme E, Pilote L. Congenital heart disease in the general population: changing prevalence and age distribution. Circulation. 2007;115:163–172. - PubMed
-
- Warnes CA, Liberthson R, Danielson GK, Dore A, Harris L, Hoffman JI, Somerville J, Williams RG, Webb GD. Task force 1: the changing profile of congenital heart disease in adult life. J Am Coll Cardiol. 2001;37:1170–1175. - PubMed
-
- Nieminen HP, Jokinen EV, Sairanen HI. Causes of late deaths after pediatric cardiac surgery: a population-based study. J Am Coll Cardiol. 2007;50:1263–1271. - PubMed
-
- Weber KT, Brilla CG. Pathological hypertrophy and cardiac interstitium. Fibrosis and renin-angiotensin-aldosterone system. Circulation. 1991;83:1849–1865. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
