

Intensity-modulated radiotherapy increases dose to the brachial plexus compared with conventional radiotherapy for head and neck cancer
- PMID: 20858665
- PMCID: PMC3473798
- DOI: 10.1259/bjr/62332495
Intensity-modulated radiotherapy increases dose to the brachial plexus compared with conventional radiotherapy for head and neck cancer
Abstract
Objective: The preferential use of intensity-modulated radiotherapy (IMRT) over conventional radiotherapy (CRT) in the treatment of head and neck cancer has raised concerns regarding dose to non-target tissue. The purpose of this study was to compare dose-volume characteristics with the brachial plexus between treatment plans generated by IMRT and CRT using several common treatment scenarios.
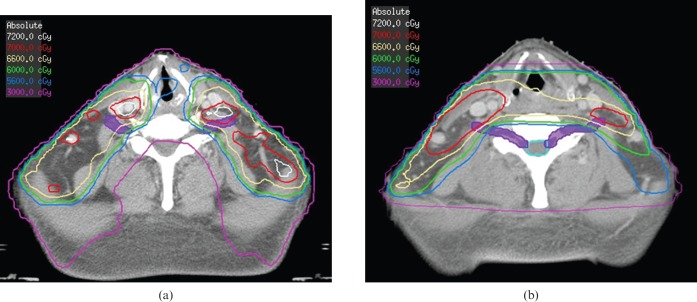
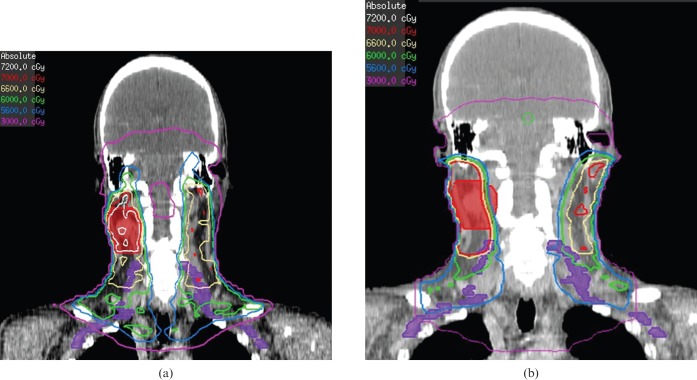
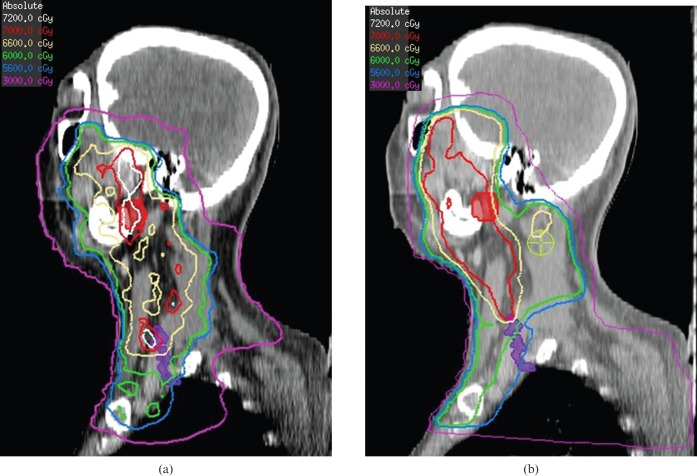
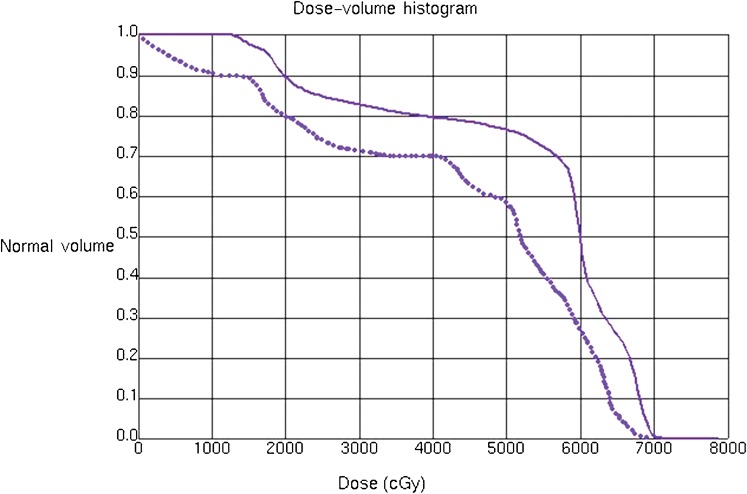
Method: The brachial plexus was delineated on radiation treatment planning CT scans from 10 patients undergoing IMRT for locally advanced head and neck cancer using a Radiation Therapy Oncology Group-endorsed atlas. No brachial plexus constraint was used. For each patient, a conventional three-field shrinking-field plan was generated and the dose-volume histogram (DVH) for the brachial plexus was compared with that of the IMRT plan.
Results: The mean irradiated volumes of the brachial plexus using the IMRT vs the CRT plan, respectively, were as follows: V50 (18±5 ml) vs (11±6 ml), p = 0.01; V60 (6±4 ml) vs (3±3 ml), p = 0.02; V66 (3±1 ml) vs (1±1 ml), p = 0.04, V70 (0±1 ml) vs (0±1 ml), p = 0.68. The maximum point dose to the brachial plexus was 68.9 Gy (range 62.3-78.7 Gy) and 66.1 Gy (range 60.2-75.6 Gy) for the IMRT and CRT plans, respectively (p = 0.01).
Conclusion: Dose to the brachial plexus is significantly increased among patients undergoing IMRT compared with CRT for head and neck cancer. Preliminary studies on brachial plexus-sparing IMRT are in progress.
Figures
References
-
- Hall WH, Guiou M, Lee NY, Dublin A, Narayan S, Vijayakumar S, et al. Development and validation of a standardized method for contouring the brachial plexus: Preliminary dosimetric analysis among patients treated with IMRT for head-and-neck cancer. Int J Radiat Oncol Biol Phys 2008;72:1362–7 - PubMed
-
- Eisbruch A. Reducing xerostomia by IMRT: What may, and may not, be achieved. J Clin Oncol 2007;25:4863–4 - PubMed
-
- Mendenhall WM, Amdur RJ, Palta JR. Intensity-modulated radiotherapy in the standard management of head and neck cancer: Promises and pitfalls. J Clin Oncol 2006;24:2618–23 - PubMed
-
- Lee N, Puri DR, Blanci AI, Chao KS. Intensity-modulated radiation therapy in head and neck cancers: an update. Head Neck 2007;29:387–400 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
